Functional reconstruction of the thumb by heterotopic thumb-to-thumb replantation and secondary opponensplasty in bilateral amputation in the upper extremities: a case report
Article information

Abstract
In traumatic amputations in the upper extremities, replantation has been commonly attempted with high success rates. However, successful replantation implies both the maintenance of length and good functional outcomes of the restored hand. Since the thumb accounts for 40% to 50% of hand function, the utmost priority is on the salvage of the thumb. In cases when replantation is not feasible, various efforts have been made to replace the thumb, including pollicization of the index finger, toe transfer, lengthening of the thumb stump, and deepening of the first web space. Alternatively, heterotopic thumb-to-thumb replantation has been suggested as a rescue plan in rare circumstances of bilateral amputation in the upper extremities. However, even if heterotopic replantation is successful, there are situations in which a severe crushing injury to the thenar muscles of the recipient’s thumb causes opposition failure of the reconstructed thumb. We report a case of functional reconstruction of the thumb in a rare case of bilateral mangling amputations in the upper extremities, by a heterotopic thumb-to-thumb replantation combined with secondary opponensplasty to compensate for the opposition failure.
Introduction
In traumatic amputations of upper extremities, replantation is commonly attempted with high success rates. However, successful replantation not only implies the survival of length but also must show good functional outcomes of the restored hand [1,2]. Hence, due to the dominant importance of thumb, accounting for 40% to 50% of hand function, the utmost priority is on the salvage of thumb. In cases when replantation is not feasible, various efforts including pollicization of the index finger, toe transfer, lengthening of thumb stump, and deepening of the 1st web space have been made.
Heterotopic thumb-to-thumb replantation is another reconstructive option applicable to rare circumstances of bilateral amputation on the upper extremity. Among bilateral mangling injuries, there are certain cases in which one hand is structurally intact but not replantable by severe proximal segment injuries, while on the other hand, the digits themselves are unsalvageable. In such cases, surgeons must try their best to restore at least one functional hand. Under these direst circumstances, there have been case reports of heterotopic thumb-to-thumb transfer as a rescue plan [1].
However, although thumb-to-thumb replantation was done, a satisfactory function of the transplanted thumb may not always be guaranteed due to the diverse level and extent of injury in different bilateral mangled hand injuries. For example, there are situations in which the concomitant damage to the intrinsic muscle causes opposition failure and disturbs the usable function of the reconstructed thumb.
We report a case of functional reconstruction of the thumb in rare case of mangling bilateral amputations on the upper extremity, by a heterotopic thumb-to-thumb replantation combined with secondary opponensplasty.
Case report
A 24-year-old man, injured by a press machine, came to the emergency room with bilateral mangling amputations on both upper extremities. The right forearm was completely amputated at proximal 1/3 level of the forearm with comminution on both ulna and radius. The amputated part had severe crushing at proximal segment but was in relatively good condition distal to wrist level with unusable thenar muscles group including abductor pollicis brevis (APB), flexor pollicis brevis, and opponens pollicis due to severe crushing and significant loss of the muscle tissue. On the other side, the nondominant left hand had crushing on the thumb, index, middle finger, and palm. The index and middle finger retained blood circulation with comminuted fractures on proximal and middle phalanges. However, the thumb was subtotally amputated without any soft tissue left for replantation and comminuted fracture at the 1st carpometacarpal (CMC) joint (Fig. 1).
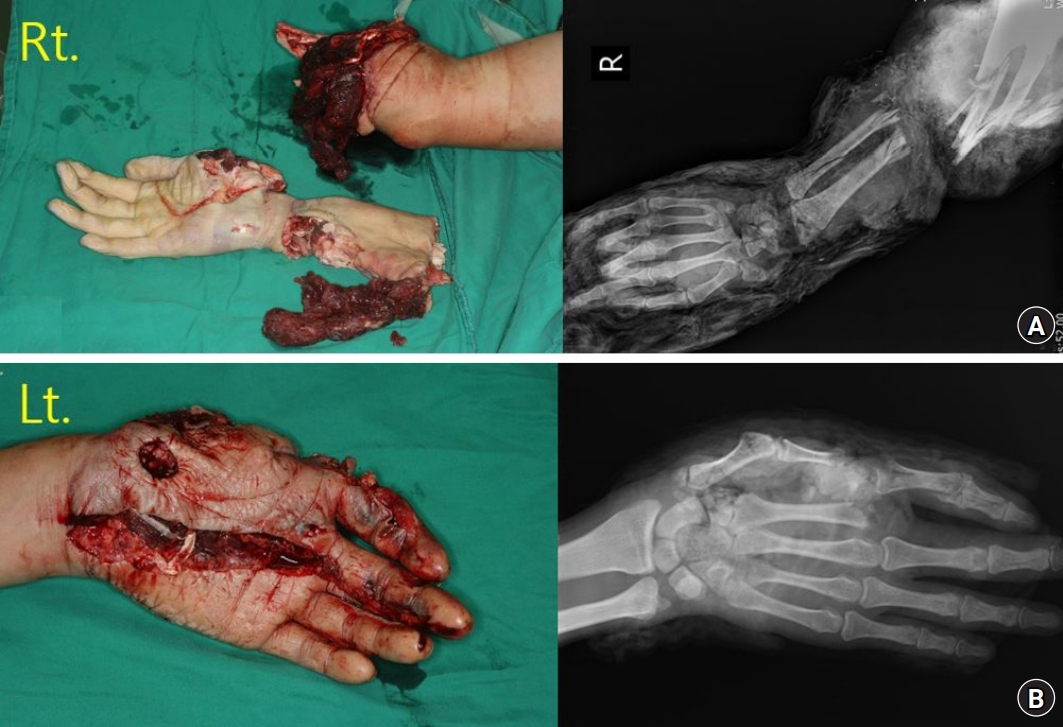
Initial preoperative photo showing bilateral mangling amputations on the upper extremity. (A) The right forearm was completely amputated at proximal 1/3 level of the forearm with comminution on both ulna and radius. (B) The nondominant left hand had crushing on the thumb, index, middle finger, and palm. The left thumb was subtotally amputated without circulation and severe crushing was found on the thenar muscles; however, the index finger retained blood circulation on the fingertips. On plain radiography, the thumb was amputated at the 1st carpometacarpal joint and the index finger showed bony amputation at proximal phalangeal head level.
Based on the comminuted, mangled nature of the right upper extremity segmental injury, we concluded that replantation of the arm is unlikely to restore a functional limb. Since the thumb of the amputated right hand was nearly intact but with crushing injury on thenar muscle, we decided to replace the unsalvageable left thumb by heterotopic thumb-to-thumb replantation. In this way, we thought we could save at least one functional hand with a thumb. The amputated right arm was planned for stump revision.
Written informed consent for publication of the clinical images was obtained from this patient.
1. Heterotopic thumb-to-thumb replantation
The right thumb was harvested at the 1st CMC joint level with extensor pollicis longus (EPL) and flexor pollicis longus (FPL) tendons, both ulnar and radial digital arteries and digital nerves, and cephalic veins. The right thumb was secured to the 1st CMC joint of the left hand by cross fixation with two 0.9 mm Kirschner wires (K-wires). EPL and FPL tendons were both repaired by core sutures in the modified Kessler technique using Ethibond 4-0 (Ethicon Inc., Raritan, NJ, USA) and multiple epitendinous sutures using PDS 4-0 (Ethicon Inc.). The damaged thenar muscles were not usable, and therefore most of the muscle tissues were trimmed. Under a microscope, both radial and ulnar digital arteries were anastomosed in end-to-end fashion with Nylon (Ethicon Inc.) 10-0, and both digital nerves were repaired by epineural interrupted sutures with Nylon 9-0. Finally, the cephalic vein and subcutaneous veins were repaired by end-to-end anastomosis as in the arteries using Nylon 10-0 (Fig. 2).
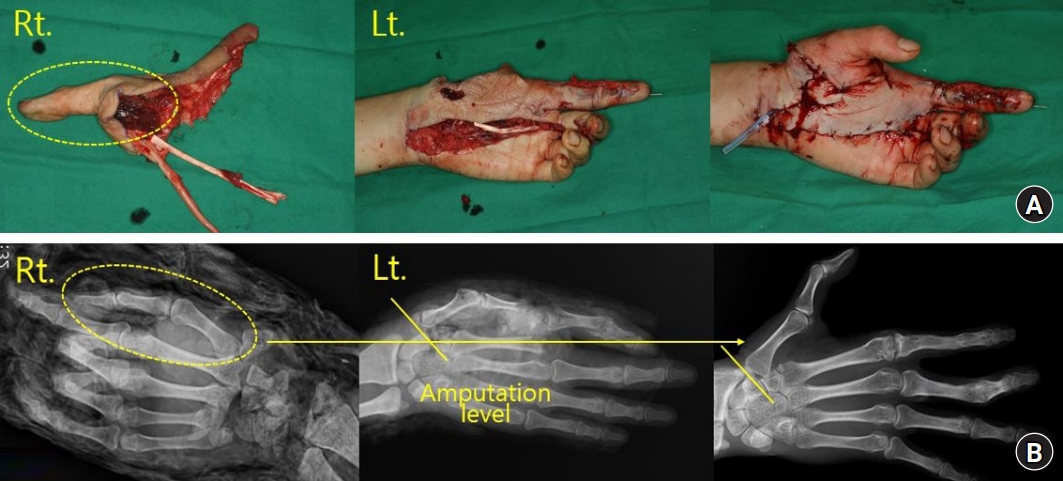
Intraoperative photo showing the heterotopic thumb-to-thumb replantation. (A) The right thumb is harvested at the 1st carpometacarpal joint level and replanted to the left hand. (B) The plain radiography taken before thumb replantation and 2 years after surgery, showing the transferred right thumb to the left hand.
The transferred thumb survived. To prevent joint stiffness, early active and passive range of motion (ROM) was encouraged from the 2nd week after surgery. After discharge, more aggressive passive exercise was done by a physical therapist three times a week at an outpatient clinic. Cross-fixated K-wires on the 1st CMC joint of thumb were removed at the 25th week after surgery.
At 2-year follow-up in the outpatient clinic, the replanted thumb had a satisfactory protective sensation. The static two-point discrimination of the thumb was 4 mm. However, opposition failure of the thumb still showed considerable limitation in daily living activities such as grabbing a bottle. The active ROM of the joints was acceptable, with 70° at the interphalangeal joint and 20° at the metacarpophalangeal joint. However, there was a significant failure in opposition with radial and palmar abduction of 30° and 25° each. The thumb could only pinch the radial side of index finger with Kapandji score of 1, and it was assessed as “fair” according to Sundaraj and Mani criteria (Table 1). By lack of opposition, the patient was not able to grab tightly or hold an object. We concluded that the injury on the thenar muscles of the replanted thumb owed for the opposition failure; hence, we planned for opponensplasty by extensor indicis proprius (EIP) transfer.
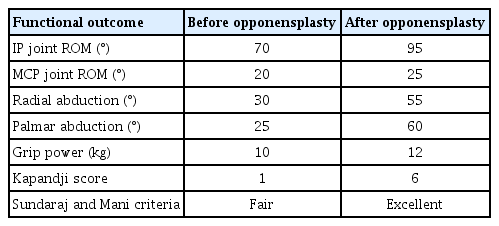
Comparison of functional outcomes of the heterotopically replanted thumb before and after opponensplasty
2. Extensor indicis proprius opponensplasty
The overall method of tendon transfer was identical to the Burkhalter technique. Due to the absence of intrinsic thenar muscles including the APB, EIP was inserted on the EPL tendon with a weaving suture using PDS 4-0 [3] (Fig. 3). Postoperatively, a dorsum protective short arm splint was applied around the thumb.
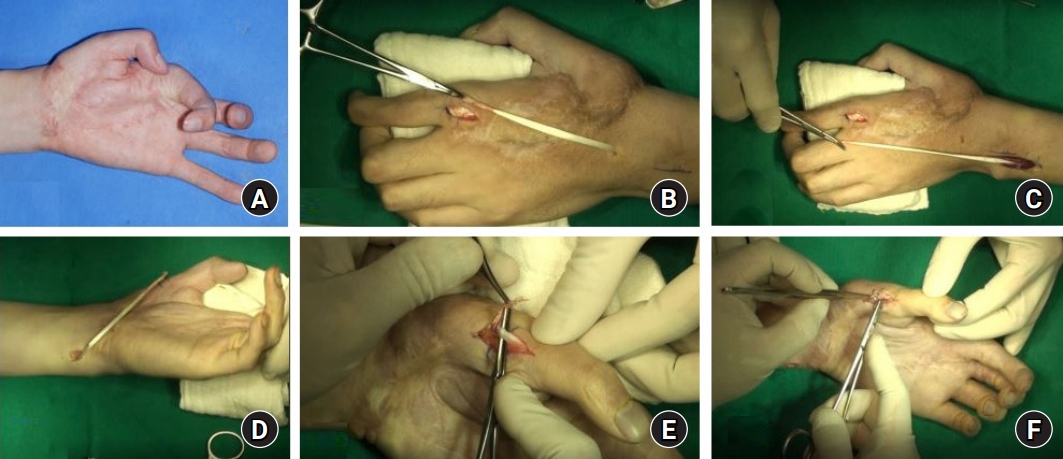
Preoperative and intraoperative photo of extensor indicis proprius (EIP) opponensplasty. (A) Preoperative photo taken at 2-year follow-up after the initial thumb replantation, showing limitations in thumb opposition. (B) The EIP tendon was identified through a linear incision over the dorsal ulnar aspect of the 2nd metacarpophalangeal joint. The tendon was detached free from the extensor digitorum communis. (C) Through wide excision of the deep fascia of forearm, the distal part of the muscle belly is gently freed and pulled out. (D) The muscle-tendon unit was tunneled through the subcutaneous border of the ulna and brought out through another incision near the pisiform. (E) Due to the absence of an abductor pollicis brevis, EIP was inserted on the extensor pollicis longus (EPL) tendon. (F) EIP was connected to EPL tendon with a weaving suture using PDS 4-0 (Ethicon Inc., Raritan, NJ, USA).
At 10-year follow-up, the opposition of thumb showed improvement. The radial and palmar abduction increased to 55° and 60° respectively (Fig. 4), and the Kapandji score increased from 1 to 4, along with the improvement in Sundaraj and Mani criteria from “fair” to “excellent” (Table 1). The patient had only minor difficulties carrying out daily living activities with DASH (Disabilities on Arm, Shoulder, and Hand) score of 28.3. He was satisfied with the surgery, and he gained full employment through driving.
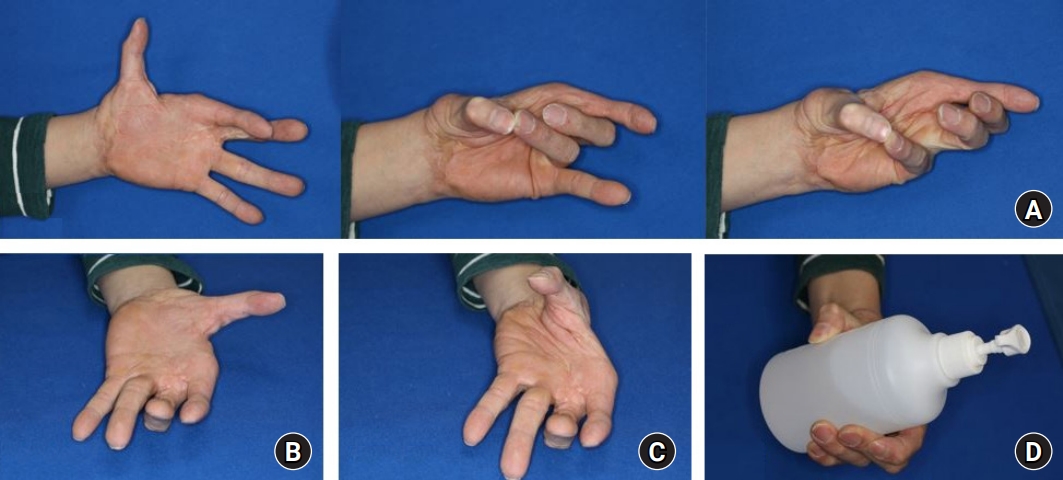
Follow-up photo of the 10th year after extensor indicis proprius (EIP) opponensplasty taken at the outpatient clinic. (A) Significant improvement in the opposition of thumb was seen, allowing the pinching on the ring and little fingers. (B) Follow-up photo of the 10th year after EIP opponensplasty taken at the outpatient clinic. (B) The radial abduction increased to 55°. (C) The palmar abduction increased to 60°. (D) The patient recovered satisfactory grip power to grab a bottle.
Discussion
In the reconstruction of hand after traumatic amputation, one should put reconstructing the thumb at top priority. The thumb accounts for the tripod pinch through opposition, and therefore, loss of thumb impairs hand function by 50% [2]. If the amputated thumb is not replantable, one should consider other options such as pollicization of the index finger, toe transfer, and deepen of the 1st web space. Still, replacing the thumb with the thumb itself is known to be more ideal in terms of cosmetics, sensory and motor function [4].
Bilateral upper extremity amputations present a rare opportunity in which heterotopic thumb replantation may be considered [1]. Cross-hand replantation was first done by Kutz et al. [4], and Tegtmeier [5] later reported the heterotopic thumb-to-thumb transfers from the nonfunctioning contralateral hand. Although rare, the reported cases have shown satisfactory pinch and grip power, with preserved opposition function when the intact intrinsic muscles and nerves are intact.
Nonetheless, there are situations where the replanted thumb is not in intact condition with severe crushing in the intrinsic muscles. In such cases, persistent opposition failure may interfere with daily living activities. In this case, severe crushing on intrinsic thenar muscles caused opposition failure, and we managed it with secondary EIP opponensplasty. Usually, EIP is inserted into the APB muscle. This is partly because the EIP tendon is usually short in length for suturing it with the EPL tendon. However, in this case, the APB muscle could not be used as an anchor, and the replanted thumb was slightly shorter than the normal thumb; hence, we made an improvisation of weaving the EIP tendon with the EPL tendon. As a result, our procedure seems to be similar to the pollicization of an index finger. Both techniques share the idea that EIP is reattached to the extensor system of thumb, serving as the EPL tendon [3]. We were able to reconstruct a functioning thumb by combining the mechanism of two surgeries: EIP opponensplasty and index finger pollicization.
A few reports have asserted that toe transfer shows great sensory recovery as good as, even better than replanted fingers [4]. This was mainly because toes are transplanted under optimal conditions with minimal ischemic time and trauma, compared to replanted fingers. The heterotopically replanted thumb in this case, showed a great recovery of sensation with static two-point discrimination of 4 mm. This was similar to two-point discrimination of less than 10 mm in toe transferred patients in average [4]. The patient showed no significant disabilities due to dullness or neurological pain in daily activities. We assume that this satisfactory sensory recovery was achieved by using intact digital nerves from the contralateral thumb, and shortening the ischemic time by implementing direct thumb-to-thumb replantation in an acute setting.
In reconstructing an amputated thumb, our case suggests that it is worth using the thumb from an unsalvageable contralateral hand, even though intrinsic muscles are severely damaged. By combining with opponensplasty, it is possible to compensate for functional deficits after heterotopic thumb replantation.
Notes
The authors have nothing to disclose.
Funding
None.