Extramammary Paget’s disease involving the bilateral axillae followed by adhesive capsulitis of the shoulder: a case report
Article information

Abstract
Few cases of bilateral axillary extramammary Paget’s disease (EMPD) have been reported. We performed surgical excision and reconstruction in a patient with bilateral axillary EMPD after consultation with dermatology. A dermatologist determined the boundaries of the lesion through Mohs micrographic surgery, and a plastic surgeon excised the lesion and reconstructed the resulting defect. Skin grafts were simultaneously performed to reconstruct the bilateral axillae. After the operation, the reconstructed site healed well, but the range of motion of both shoulders was reduced. After referral to a doctor specializing in rehabilitation, the patient was diagnosed with adhesive capsulitis and received additional treatment. Since no previous reports have presented a case of adhesive capsulitis after the reconstruction of bilateral axillary EMPD using skin graft, this case is noteworthy.
Introduction
Extramammary Paget’s disease (EMPD) is characterized by erythematous lesions with clear borders and commonly occurs on the genitalia, perianal region, scrotum, penis, and axillae. EMPD accounts for 6% to 7% of all cases of Paget’s disease, and only hundreds of cases have been reported worldwide [1,2]. Furthermore, axillary EMPD is exceedingly rare, and, to date, very few reports have presented cases of bilateral axillary EMPD. In particular, no published studies have described the postoperative complications of surgery to treat bilateral axillary EMPD.
Adhesive capsulitis (AC) is a shoulder disease characterized by pain and reduced motor function [3]. Pathologically, it involves chronic inflammation of the synovial capsular layer that leads to capsular thickening and fibrosis. AC affects 3% of the world’s population and is disproportionately common among women aged 40 to 70 years [3]. Although the etiology of AC remains unclear, orthopedic shoulder surgery following trauma has been suggested as a potential cause [3].
This report presents a case of AC that occurred after surgical treatment of bilateral axillary EMPD, a very rare disease. Through this case, we hope to raise clinicians’ awareness regarding the possible occurrence of AC as a complication after surgical treatment of bilateral axillary EMPD. Informed consent was obtained from the patient for data publication, including the use of images.
Case report
A 49-year-old female patient had erythematous patches on both axillae about 1 to 2 years ago that suddenly grew, prompting her to visit our dermatology department (Fig. 1). The patient was diagnosed with EMPD based on biopsy findings and was promptly referred to the plastic and reconstructive surgery department for surgical excision and reconstruction of the bilateral axillae. The patient had no other abnormalities or diseases. After a discussion with the patient, the authors decided to reconstruct both axillae by skin grafting at the same time after removing the lesions. On the day before surgery, the authors removed the lesions based on the margin confirmed by the dermatologist through Mohs micrographic surgery. After excision, the lesions were sent for permanent biopsy. The histological and immunohistochemical findings are presented in Fig. 2. Microscopically, single or clustered cells confined to the epidermis—usually above the basal layer of the epidermis—called Paget cells were identified. These cells can be morphologically distinguished from squamous epithelial cells by the presence of a pale to eosinophilic cytoplasm and large, pleomorphic nuclei with conspicuous nucleoli (Fig. 2A, 2B). Immunohistochemical staining for cytokeratin 7 also visualized them with positive cytoplasmic staining (Fig. 2C). The histologic findings of both lesions (left and right) were identical to each other. The defect in the right axilla measured 9×8 cm and that in the left axilla measured 8×8 cm. Reconstruction was performed using split-thickness skin grafts after applying a SureDerm acellular dermal matrix (Hans Biomed Corp., Seoul, Korea) to reduce postoperative contracture. As dressing for the skin graft site, an ointment-impregnated gauze was first applied, and then negative-pressure wound therapy (Curavac; Daewoong Bio, Inc., Seoul, Korea) was applied. To promote engraftment, the patient’s shoulders were kept elevated and abducted by placing both hands above her head for 7 days (Fig. 3). After surgery, the patient started to report shoulder pain, but the posture was maintained for 7 days. After removing the Curavac on the 7th day after surgery, the range of motion (ROM) was checked, and it was confirmed that the ROM had decreased. One month after surgery, the patient’s right shoulder showed angles of forward flexion, abduction, internal rotation, and external rotation of 80°, 45°, 50°, and 0°. The corresponding values for the left shoulder were 150°, 150°, 40°, and 0°. The patient was referred to a physician specializing in rehabilitation medicine and was diagnosed with AC based on the clinical and ultrasound findings (Fig. 4).

Preoperative picture showing extramammary Paget’s disease in the bilateral axillae. The patient visited our clinic with bilateral axillary erythematous brownish patches that had developed 1 to 2 years ago.

Microscopic findings of extramammary Paget’s disease. (A, B) Hematoxylin and eosin-stained slides (A, ×100; B, ×400). (C) Immunohistochemical staining for cytokeratin 7 (×400).

Posture of the patient maintained for 7 days after skin graft surgery. The patient maintained shoulder elevation and abduction with both hands above the head.
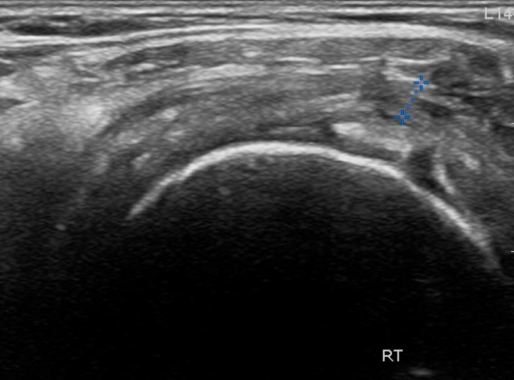
Ultrasonography of the shoulder area performed 1 month after surgery. On ultrasonography, capsular thickening in the synovial capsular layer was confirmed, and adhesive capsulitis was diagnosed with physical symptoms.
The grafted sites successfully healed within 3 months after surgery (Fig. 5). At 6 months after surgery, in the right shoulder, the angles of forward flexion, abduction, internal rotation, and external rotation were 150°, 120°, full, and 45°, respectively. The corresponding values for the left shoulder were 150°, 120°, full, and 45°, respectively. EMPD did not recur during the 1-year follow-up period. The patient was treated with nerve blocks, steroid injections, medications, physiotherapy, and manual therapy for AC as prescribed by the rehabilitation specialist. At 1 year postoperatively, the patient’s restricted ROM had not completely resolved (Fig. 6).
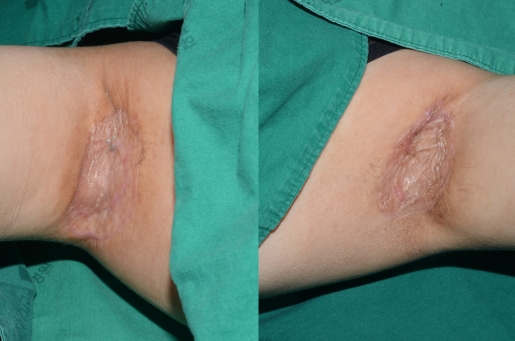
A photograph taken 3 months after surgery, showing successful healing of the skin grafts in both axillae.

After 1 year of treatment at the Department of Rehabilitation Medicine, the range of motion had still not fully recovered.
Discussion
EMPD is a type of intraepithelial adenocarcinoma. The first reported case of EMPD was detected on the male genitalia by Crocker in 1889 [4]. It usually occurs in the perineum, which contains abundant apocrine sweat glands. The most commonly affected sites vary between Western and Asian populations. In Western populations, EMPD most commonly occurs on the labia majora, followed by the perianal region, scrotum, penis, and groin. However, in Asians, EMPD is more common among men and most commonly affects the scrotum and penis [5]. EMPD confined to the axilla is very rare; only three cases of bilateral axillary EMPD have been published worldwide, and no previous cases from Korea have been reported [6].
AC, also known as “frozen shoulder,” is pathologically characterized by contracture of the glenohumeral capsule accompanied by pain and reduced ROM in the glenohumeral joints. The disease course of AC is traditionally divided into the painful, freezing, and recovery stages; however, there is no evidence to support this staging, and its clinical utility is questionable. Although the causes of AC are unclear, it is associated with diabetes mellitus, rotator cuff tendinopathy or tears, subacromial bursitis, biceps tendinopathy, recent shoulder surgery or trauma, and inflammatory diseases [3,7]. The accurate diagnosis and early treatment of AC help to reduce pain and increase ROM. Therefore, physicians must be aware of the possibility of AC in patients with a history of the aforementioned diseases or in those who have undergone surgery around the glenohumeral joint. Before undergoing surgery, patients should also be informed of the risk of AC. In addition, postoperative shoulder abduction and elevation were performed to promote stability of the skin grafts. A previous study reported that the axillary nerve shortened when shoulder abduction and elevation position were performed. In this case, the patient experienced pain in the shoulder abduction and elevation posture, which induced axillary nerve stretching, potentially leading to neuropathy. However, it would be difficult to prove a clear causal relationship [8].
Skin grafts or flaps can be used to reconstruct axillary defects. The thoracodorsal artery perforator (TDAP) flap can be considered as the first option to preserve full ROM of the shoulder and obtain satisfactory cosmetic outcomes. However, since it is difficult to maintain the necessary posture during surgery when reconstructing a defect in the bilateral axillae, a TDAP flap may not be an appropriate choice when both sides are to be operated at once. Therefore, the authors planned reconstruction with skin grafts, and used acellular dermal matrix to prevent scar contracture after skin grafting. After surgery, both hands were placed above the head and the shoulder was maintained in elevation and abduction for 7 days, and the skin was successfully engrafted.
Although a previous study reported that AC occurred in 11% of cases after shoulder surgery, the mechanisms underlying postoperative AC remain unclear [7]. Postoperative AC has been an important topic of discussion among orthopedic surgeons. Another study reported that approximately 7% to 10% of patients developed AC after breast cancer surgery, and the risk of AC was found to be higher in patients aged 50 to 59 years [9]. As in this case, the prolonged maintenance of shoulder abduction to prevent scar contracture may be a cause of AC. However, after reconstructing EMPD in both axillae at once with skin grafts, as in our case, maintaining shoulder fixation to prevent scar contracture was necessary.
AC significantly compromises the patient’s quality of life by causing pain and reduced motion. Early diagnosis and treatment can help reduce pain and increase ROM. Thus, an awareness of the possibility of AC can positively contribute to its management. Given that bilateral axillary EMPD is rare, with no existing reports on the use of skin grafts for the reconstruction of such cases, we were not able to predict the development of AC in our patient. However, in light of our experiences, in subsequent cases where an attempt is made to reconstruct EMPD that occurred in both axillae by skin grafts, it is necessary for the operator to recognize the risk of AC occurrence and to provide a sufficient explanation to the patient.
We reported a case of EMPD confined to both axillae that was successfully treated by the surgical removal of lesions and reconstruction using skin grafts; however, postoperative AC developed. The present case, therefore, demonstrates the need to consider the possibility of AC following bilateral axillary EMPD removal and reconstruction using skin grafts.
Notes
The authors have nothing to disclose.
Funding
This work was supported by clinical research grant from Pusan National University Hospital in 2020.