양측 슬관절 주위 절단의 성공적인 재접합술: 증례 보고
Successful Replantation after Amputation around Both Knee
Article information

Trans Abstract
Reducing ischemic time is the most important factor associated with good results in major limb replantation. This case describes the surgery and outcome of replantation of both major limbs in a patient with amputation of both lower extremities due to rope entanglement on a ship. Emergency surgery restored circulation in 3 hours and 40 minutes after amputation on the left side, and 4 hours and 50 minutes after amputation on the right side. The left knee of the patient had undergone joint fusion and the right knee could move from 0 degree to 100 degrees. At present, the patient is able to walk using crutches. These results demonstrate that good results can be obtained if bilateral anastomosis is possible in both knees.
Introduction
Patients who visit a hospital with major limb amputation must choose between revision and replantation [1]. Replantation of both lower extremities has a low success rate and less satisfactory functional results. Minimizing ischemic time in major limb replantation is crucial for better results. Major limb replantation with ischemia time greater than 6 hours may lead to reperfusion syndrome. Even if blood flow is maintained by replantation, necrosis can occur, requiring amputation. In particular, high-level amputated parts with high muscle mass require restoration of blood flow within four hours of warm ischemia time [2]. Therefore, in cases requiring replantation of both major limbs, it is difficult for a single surgical team to determine whether to proceed with replantation of both lower extremities. The present case report describes the successful replantation surgery of both major extremities by a single surgical team and provides a discussion of the results. The patient was informed that data concerning the case would be submitted for publication, and he provided consent.
Case Report
The patient was a 62-year-old man who visited the hospital with amputation of both lower extremities due to rope entanglement on a ship (Fig. 1). After the patient’s arrival in the emergency room, radiological examination showed amputation of the right and left legs 15 cm above and 5 cm below the knee joints, respectively. As the parts below both amputated knee joints were in good condition, replantation of both extremities was planned. The emergency surgery started 2 hours and 10 minutes after the patient’s arrival at the hospital. After induction of general anesthesia, the patient was placed in a prone position. Starting from the right amputated part, which was in good condition, we identified the popliteal artery and vein from the proximal and distal stumps and marked them with a clip. To minimize the ischemia time, we cut the bone to 5 cm adjusted to the axis of the bone at the fracture site of the femur and performed fixation to the femur with two Steinman pins. We then repaired the popliteal artery by end-to-end anastomosis and monitored blood circulation at an ischemia time of 3 hours and 40 minutes. We wrapped the right amputated part with gauze and bandages and started exploration of the left amputated part, which was in worse condition. The popliteal artery and vein were also marked with a clip. Five centimeters of the proximal fracture of the tibia at the knee joint was removed, and fixation was temporarily performed with a single Steinman pin because the bone anchoring was not yet properly performed. The popliteal artery was repaired by end-to-end anastomosis, and blood circulation was monitored at an ischemia time of 4 hours and 50 minutes. A total of 8,400 mL of blood was transfused during surgery.

A 62-year-old male patient visited the hospital with amputation of both lower extremities due to rope entanglement on a ship.
After checking the circulation in both extremities, a blood clot in the popliteal vein of the right amputated part was removed, and venous anastomosis was performed. After the damaged tibial nerve was removed, neurorrhaphy was performed. Similarly, the blood clot in the popliteal vein of the left amputated part was also removed, and venous anastomosis was performed. The damaged tibial nerve was also removed and neurorrhaphy was performed. The amputated parts of both extremities were debrided, and the bleeding was controlled. The damaged muscles were arranged and myorrhaphy, ligament repair around the knee joint, and suturing were performed. An external fixator was used in a prone position due to the unstable fixation of the fractured part (Fig. 2A, 2B). Postoperatively, the body temperature was maintained using a warming cover, and heparin 25,000 IU was added daily to prevent pulmonary thrombosis. Patients were monitored for posterior tibial arterial pulse using Doppler ultrasound.
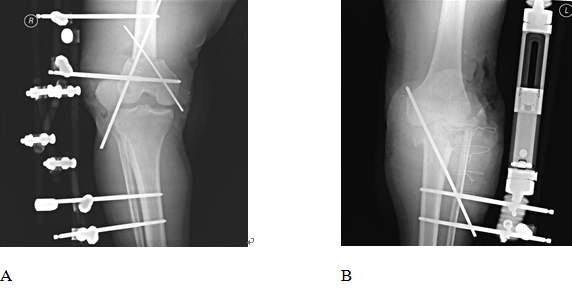
(A) Radiographs of the right knee after surgery showing the 5-cm shortening at the tibial proximal fracture of the femur fixed with a Steinmann pin. An external fixator was used. (B) Radiographs of left knee after surgery showing that the tibia proximal shaft fracture was removed by 5 cm and fixed with a Steinmann pin. An external fixator was used.
Two weeks after surgery, segmental necrosis occurred (Fig. 3). The necrotic portions were excised and treated with skin grafts. Arthrodesis of the left knee joint was performed. Three months after the initial surgery, the soft tissue damage had fully recovered. The external fixator was removed and a retrograde intramedullary nail was inserted in the right distal femoral fracture.

Image 2 weeks after surgery showing necrosis around the left knee joint.
Bone union was confirmed 2 years after the operation (Fig. 4A–4C). While the left knee joint was fixed, the active range of motion of the right knee joint was 0–100 degrees. The patient was able to walk with crutches. There was no pain, but nerve transplantation was considered due to left lower limb sensation.

(A) Image 2 years after surgery showing no problems with the appearance of the replanted parts. (B, C) Radiographs 2 years after surgery showing synostosis at the supracondylar fracture of the right femur and fixation of the left knee joint.
Discussion
Along with an increase in the number of patients with high-energy injuries, there has been an increase in the number of patients requiring amputation of major limbs [3]. In addition, people in Korea have a strong demand for replantation in cases of limb amputation as they are influenced by the Confucianism belief that emphasizes the preservation of the four limbs. However, only selected tertiary care centers or special hospitals perform such procedures. Therefore, patients seeking hospitals with facilities to perform replantation may increase ischemic time and lead to unsatisfactory results after replantation surgery. The continued development of prostheses has resulted in increased patient demand for functional results after replantation, which consequently increases the demand for satisfactory results.
Studies on replantation of both extremities have reported satisfactory results in children [4] and a few reports on replantation of both ankles in adults [5]. However, these studies dealt with the replantation of both extremities by two surgical teams rather than a single surgical team, as in the present case. Moreover, comparison of replantation of both extremities to prosthetics of both extremities indicated higher patient satisfaction for replantation [6]. Therefore, if patients agree, replantation of both extremities is worth attempting.
Patients with amputation of both extremities should decide whether to have replantation of one or both legs. There are also reports considering crossover replantation on the leg in better condition [7]. In other words, lower leg replantation is difficult and vascular anastomosis may not be possible depending on the condition of the amputated parts, which requires the consideration of various factors before deciding to perform replantation [1].
Good results in limb replantation require minimizing the perioperative warm ischemic time of the amputated part [2]. This is even more important in replantation of both extremities. Therefore, two surgical teams performing replantation of both legs simultaneously is optimal. However, if not possible, replantation by a single surgical team places significant pressure on surgeons like the researchers. Recently, temporary vascular shunts have been frequently attempted to save the amputated major limb [8]. In the present case, the distal femoral fracture was initially fixed with a Steinmann pin on the right lower limb, which was in better condition than the left lower limb. Second, the artery was anastomosed. Then, the bone of the left lower limb was fixed with a Steinmann pin while the artery anastomosis was performed in order to reduce the ischemic time of both legs. After securing the circulation of both legs, venous anastomosis, neurorrhaphy, myorrhaphy were performed, in that order, while checking the patient’s condition.
Unlike limb replantation in other parts, the outcome of replantation around the knee joint depends on the patients’ satisfaction with recovering knee joint mobilization. In this case, because shortening of the bone of the right amputated part was possible without damaging the knee joint, syndesmorrhaphy of the joint around the knee was performed for recovery of the joint. If the amputated part is close to the knee joint, as occurred in the left part of the patient in the present case, vascular anastomosis is possible by removing the proximal tibia of the amputated part rather than bone shortening. Instead, arthrodesis was performed. Unexpectedly, the patient had a higher level of satisfaction with the left knee joint, in which bone fixation had been performed, because, while the right knee had joint mobility, it was unstable.
Successful replantation after amputation of both extremities ideally involves two surgical teams to perform replantation simultaneously reducing perioperative warm ischemic time. However, if this is not possible, it is important to quickly perform artery anastomosis of the opposite leg after artery anastomosis of the leg in better condition.
Notes
The authors have nothing to disclose.
Acknowledgements
This work was supported by clinical research grant from the Medical Research Institute, Pusan National University Hospital.