Introduction
Recurrent subluxation or dislocation of the extensor carpi ulnaris (ECU) tendon from the ulnar groove is an important cause of pain at the dorsoulnar side of the wrist [1,2]. Symptomatic recurrent subluxation of the ECU tendon has become increasingly recognized since its description in 1964 [3]. It is typically reported in young athletes who play racket or stick sports such as tennis, golf, and baseball. Forceful wrist supination, flexion, and ulnar deviation may result in rupture of the ECU tendon sheath or volar subluxation of the tendon out of the distal ulnar groove within a redundant sheath [4-7].
The ECU tendon lies in an ulnar groove and is contained by a separate fibro-osseous subsheath, of which the medial attachment is reinforced by the fibrous linea jugta, which resists medial and volar subluxation [8,9]. Various techniques of ECU tendon sheath reconstruction have been described for treatment of ECU tendon sheath subluxation [1,4,5,10]. Among them, The anatomic reconstructive surgery of ECU subsheath has emerged as a treatment for ECU instability, demonstrating positive clinical outcomes including range of motion (ROM) of the wrist joint, grip strength, and patient satisfaction [8].
The ECU instability is found more frequently among patients with vulnerability in distal ulnar morphology [11]. However, subluxation of the ECU tendon is frequently observed on imaging, but it is unclear whether this is clinically relevant—particularly when there are no ulnar-sided symptoms and there is no clinical concern for ECU tendon instability [12-14]. The relationship between symptomatic development and distal ulnar morphology has not been clearly elucidated.
The purpose of this study is to determine the outcome of anatomic ECU subsheath reconstruction and the effects of distal ulnar morphology on symptomatic ECU subluxation in patients operated on in our hospital. The evaluation involves an examination of the radiological and clinical findings in relation to the prediction that distal ulnar morphology will influence symptomatic ECU subluxation.
Methods
Ethics statement: This study was approved by the Institutional Review Board of Konkuk University Medical Center with the informed consent of the patients (No. KUMC 2020-07-095).
1. Patients
This was a retrospective study involving patients who underwent anatomic ECU subsheath reconstruction due to symptomatic ECU subluxation from January 2015 to July 2018 and were followed up for more than 6 months. One surgeon performed the surgery, and this was a single center study.
Symtomatic ECU subluxation was diagnosed based on positive ECU tenderness and swelling and ECU synergy test and a clicking sound from the ECU during wrist rotation and ulnar deviation on physical examinations performed on a patient who visited the clinic with dorsoulnar side wrist pain based on medical history. According to medical history, all patients had no clearly remembered history of trauma before the onset of the symptoms. In addition, all patients had hobbies such as gym, golf, tennis or had a high level of physical activity. Magnetic resonance imaging (MRI) was performed on those patients. And we confirm symptomatic ECU subluxation.
Those patients were first fixed in the short-arm splint in radial deviation and slightly extension, and supination movements were instructed to be limited with medication. After 4 to 6 weeks of splinting, education was given to limit movement to induce subluxation. We observed the improvement of the patient’s symptoms for 3 months, and those whose clinical symptoms did not improve or worsened after 3 months of conservative treatment underwent surgical treatment (anatomic ECU subsheath reconstruction).
Study subjects were 12 wrist joints of 12 patients. The mean postoperative follow-up period was 6 months (median, 6.4 months; range, 4–12 months), including a clinical evaluation conducted before the operation and at the final follow-up for comparison. Patients included eight males and four females; affected wrist joints were on the right arm in seven cases and on the left arm in five cases. The mean age was 39 years (range, 19–70 years).
A control group was selected to determine the effects of distal ulnar morphology on symptomatic ECU subluxation. Group 1 was 12 patients who underwent anatomic ECU subsheath reconstruction due to symptomatic ECU subluxation, group 2 was 24 patients with asymptomatic ECU subluxation, and group 3 was 24 patients without symptoms or subluxation in the ECU.
The control group (groups 2 and 3) were collected at patients who underwent MRI to find the focus of wrist pain other than ECU problem. If there were no symptoms but ECU subluxation was found on MRI, they were group 2. If there were no problems on ECU, they were group 3.
2. Radiologic and clinical evaluation
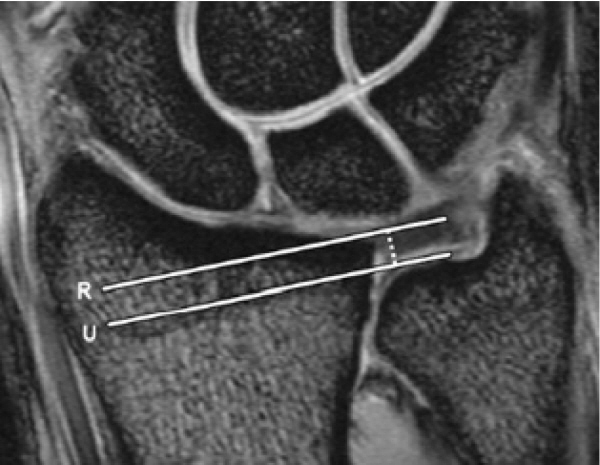
Assessment included MRI for an evaluation of distal ulnar morphology and the measurement of ulnar variance, ulnar styloid length, and ECU groove depth using the methods shown in Figs. 1 to 3, respectively. The association between distal ulnar morphology and symptomatic ECU subluxation was examined by comparing measurements for three groups: group 1 (with 12 cases of symptomatic ECU subluxation), group 2 (with 24 cases of non-symptomatic ECU subluxation), and group 3 (with 24 normal cases with no ECU subluxation).
The clinical evaluation of anatomic ECU subsheath reconstruction included a comparison between before the operation and at the final follow-up using the Patient-Related Wrist Evaluation (PRWE) score, the Disabilities of the Arm, Shoulder, and Hand (DASH) score, grip strength, and the ROM of wrist joint.
3. Surgical methods and follow-up
The anatomic ECU subsheath reconstruction was conducted using the conventional method (Fig. 4) including a 1.0-mm JuggerKnot anchor (Biomet, Warsaw, IN, USA) in subsheath reconstruction without deepening the hole in the ECU. Postoperative care included a long-arm splint in semipronation for 2 weeks, and a long-arm cast in the same position after suture removal, which was replaced by a short-arm splint in the 5th week. From that point, patients were allowed to flex and extend the operated arm, followed by pronation and supination in the 8th week, and exercise in the 3rd month. The final follow-up, 6 months after surgery included ultrasound to determine the status of ECU subluxation. No patients showed ECU subluxation.
4. Statistical analysis
The comparison of the three groups in ulnar variance, ulnar styloid length, and ECU groove depth was conducted using the Kruskal-Wallis test. Afterwards, the Bonferroni method was used to confirm significant differences between each group. The clinical evaluation of anatomic ECU subsheath reconstruction involved performing the Wilcoxon signed-rank test on preoperative and postoperative DASH score, PRWE score, grip strength, and ROM before and at final follow-up, using SAS ver. 9.4 (SAS Institute Inc., Cary, NC, USA). The statistical significance level was defined as the case where the p-value was less than 0.05.
Results
According to the MRI findings, the mean ulnar variance was 1.5 mm (range, –1.0 to 3.0 mm) for group 1, 0.6 mm (range, –2.0 to 1.0 mm) for group 2, and 0.4 mm (range, 0–1.0 mm) for group 3. The mean ulnar styloid length was 4.6 mm (range, 4.0–5.3 mm) for group 1, 5.2 mm (range, 4.2–7.0 mm) for group 2, and 4.7 mm (range, 3.7–5.6 mm) for group 3. The mean ECU groove depth was 2.0 mm (range, 1.3–3.0 mm) for group 1, 1.3 mm (range, 1.0–1.4 mm) for group 2, and 2.1 mm (range, 1.2–3.4 mm) for group 3. Ulnar variance and ulnar styloid length and ECU groove depth was significantly different between the three groups through the Kruskal-Wallis test (Table 1). Through this, it was possible to interpret that at least on group was different.
To interpret the statistical results, a post hoc analysis using the Bonferroni method showed that ulnar variance showed a statistically significant difference between group 1 and group 2, and ECU groove depth showed a statistically significant difference between group 1 and group 2, as well as between group 2 and group 3. Ulnar styloid length showed no statistically significant difference in any group as a result of post hoc testing (Tables 2–4).
A comparison between preoperative and postoperative clinical results in symptomatic ECU subluxation showed no statistically significant change in the range of flexion (57° to 56°) and extension (53° to 51°) in the wrist joint. However, the ROM in pronation (79° to 85°) and supination (75° to 85°) significantly increased. Grip strength, DASH score, and PRWE score also significantly changed. Table 5 and Fig. 5 shows an increase in the median grip strength of the affected hand from 28 kg (interquartile range [IQR], 19–34 kg) to 33 kg (IQR, 26–40 kg), a decrease in DASH score from 40 to 9, and a decrease in PRWE score from 48 to 12. No patients showed postoperative wound infection or nerve damage due to complications, persisting clinical symptoms, or relapse, or were readmitted for primary concerns of another rupture.
Discussion
This study aimed to determine the outcome of anatomic ECU subsheath reconstruction and evaluate the effects of distal ulnar morphology on symptomatic ECU subluxation. Our results demonstrate positive outcomes of anatomic ECU subsheath reconstruction. It was confirmed that patients who underwent anatomic ECU subsheath reconstruction had improvements in DASH, PRWE score, grip strength, and supination-pronation ROM compared before surgery.
And among distal ulnar morphology, Ulnar variance showed a statistically significantly larger ulnar negative variance in the symptomatic ECU subluxation group compared to the asymptomatic ECU subluxation group. Ulnar styloid length showed no statistically significant difference in any group as a result of post hoc testing. ECU groove depth in the asymptomatic ECU subluxation group was shallower than normal group, but on the other hand, the symptomatic ECU subluxation group was found to be deeper than the asymptomatic ECU subluxation group.
The distal ulna is intimately associated with ECU tendon, which travels in the ECU groove of the distal ulna for approximately 15 to 20 mm and is covered by the ECU subsheath and retinaculum [12]. Previous research has shown that that distal ulnar morphology influences subluxation and pathology of the ECU tendon [11,15]. Specifically, studies have reported that ECU subluxation and ECU tendon pathology increase as ulnar negative variance increases, that ECU groove depth and length are negatively associated with ECU subluxation while showing no direction relationship with ECU tendon pathology, and that ulnar styloid length is not directly related to either ECU subluxation or ECU tendon pathology [15].
In our study, we obtained significant results comparing distal ulnar morphologic parameters between groups. It was verified that as ulnar negative variance increases symptomatic ECU subluxation occurs. Asymptomatic ECU subluxation occurs as the ECU groove depth becomes shallower, but symptomatic ECU subluxation was found to be more frequent at groove depths closer to normal. This provides supportive evidence for effect of distal ulnar morphology on ECU tendon and indicating the need for the pathoanatomical re-evaluation of ECU subluxation.
The ECU tendon travels in a fibro-osseous tunnel with the floor being the ECU groove and the roof being the tendon subsheath [15]. Therefore, if there is a problem with the fibro-osseous tunnel (ECU groove or/and subsheath) occurs with the constraint of the ECU tendon.
In our study, according to history taking, the onset of symptoms in all patients was not caused by a one-time trauma but rather by high-level activity (sports or jobs). And according to the surgery findings, all cases showed a tear in the subsheath and periosteal stripping of ulnar leaf, type C in the Inoue and Tamara classification [5], which suggests that the subsheath is the primary pathoanatomical structure. In particular, the location of the ulnar side tear suggests that the damage to the labral attachment of the ulnar leaf in subsheath is the primary pathoanatomical structure of the ECU subluxation, as Graham’s study demonstrated [16].
We hypothesized that the cause of symptomatic ECU subluxation is anatomically periosteal stripping of the ulnar leaf of the subsheath due to repetitive ECU subluxation inducing movements and ulnar negative variance increase the angular trajectory of ECU tendon, making it vulnerable to medial forceful vectors. A shallower osseous groove can also put a burden on ECU stability. However, we concluded based on the results of this study, it was verified that the pathophysiology of symptomatic ECU subluxation is unrelated to ECU groove depth.
Many surgeons consider a shallow ulnar ECU groove a source of symptomatic ECU subluxation [8] and therefore deepen the groove as a component of ECU surgical stabilization [17]. However, In cadaveric study, groove deepening did not improve stability of the ECU tendon compared with the reconstructed subsheath, and reconstruction alone was equally effective at eliminating dislocation event [18]. Even other studies have reported negative impacts of ECU groove deepening, such as consequence of bone weakened during procedure leads to rim fracture and greater propensity to recurring subluxation [16]. The results of our study also do not recommend additional bone procedures.
Therefore, suturing the ECU subsheath to its original position, anatomic reconstruction can be expected to produce good clinical results. Additionally other surgical procedures such as groove deepening are not necessary. And our study also demonstrated positive outcomes on all clinical indicators and no unusual complications in all cases of anatomic ECU tendon sheath reconstruction, leading to the conclusion that the anatomic ECU tendon sheath reconstruction can be used as the primary surgical technique for patients with symptomatic ECU subluxation.
Limitations of this study include the small sample size (of 12 cases) from a limited pool of patients and a relatively short follow-up period (of 6 months on average). And it is difficult to discuss the superiority of our surgical technique since it is not compared with other surgical techniques. Future studies need to include more cases and longer follow-ups and comparison of surgical techniques.
Conclusion
Among distal ulnar morphology, negative ulnar variance is associated with symptomatic ECU subluxation, and shallow ECU groove depth affects asymptomatic ECU subluxation but is unrelated to symptoms. And anatomic ECU tendon sheath reconstruction is an effective surgical method in stabilizing the ECU and in terms of clinical outcomes.