Introduction
The metacarpal fracture is one of the most common types of hand fractures, accounting for approximately 33% to 42% of all hand fractures [1,2]. Furthermore, the fifth metacarpal neck fracture (Boxer’s fracture) is the most common metacarpal fracture, ranging from 25% to 55% of all metacarpal fractures [3,4]. Patients at risk for the fifth metacarpal neck fracture are usually young men who engage in aggressive behavior or heavy sports activities that can result in pressure on the knuckles in a clenched fist [5,6]. Most of the fifth metacarpal neck fractures can be treated with nonoperative treatment, but when open fractures, significant angulation, malrotation, comminution, or intraarticular extension exist, surgical treatment is recommended to prevent residual deformity and functional disability [7,8].
In many currently used surgical techniques for boxer’s fracture [3,9,10], antegrade intramedullary Kirchner wire (K-wire) fixation (Bouquet pinning) is a common surgical method. In this technique, two or three K-wires between 0.8 and 1.2 mm in diameter are inserted from the proximal metaphysis and pass through the intramedullary portion, and finally fix the distal fragment across the fracture site in a bouquet-like fashion [9,11-13]. The advantages of this technique are minimally invasive, ease of operation, and most of all, early joint motion is possible because there is no K-wires or implant around the metacarpophalangeal joint [8,14].
The bouquet technique using pre-bent K-wires act on a three-point intramedullary fixation, providing accurate reduction and adequate fracture site stability [15]. The blunt distal tip of the K-wire should be positioned at the intact portion of the distal fracture fragment for the stable three-point fixation. However, many of the fifth metacarpal neck fractures are frequently accompanied by comminution around the fracture site and its head and neck, making it challenging to get a firm three-point fixation [8]. Therefore, understanding the configuration and characteristics of the comminuted fifth metacarpal neck fracture is essential for successful operative treatment, especially for the antegrade intramedullary K-wire fixation.
This study aims to investigate the characteristics and shape of the comminuted fragment in the fifth metacarpal neck fracture and suggest the appropriate K-wire position and surgical methods.
Methods
Ethics statement: The Institutional Review Board of Korea University Anam Hospital approved the protocol of this study (No. 2022AN0390), The study was performed in accordance with the Declaration of Helsinki, and written informed consent was waived due to its retrospective nature.
We conducted a retrospective review for all patients diagnosed with the fifth metacarpal neck fractures from January 2010 to April 2022 at our institution. We enrolled 41 consecutive patients 18 years and older who had a computed tomography (CT) scan following the diagnosis of the fifth metacarpal neck fractures on plain radiographs. The exclusion criteria were as follows: (1) the fifth metacarpal head and shaft fractures, (2) the patients who did not undergo CT scans, and (3) cases with open growth plates visible on plain radiographs.
1. Operative methods
Percutaneous pinning across the fracture [16], antegrade intramedullary pinning [9], retrograde intramedullary pinning [10], and plate fixation were performed under fluoroscopy for the fifth metacarpal neck fracture in our institution. Besides plate fixation, the above three surgical methods are to fix the proximal and distal fragments using K-wires. For crossed pinning, two or more K-wires were introduced percutaneously from the proximal or distal fragment crossing the fracture site to fix the metacarpal head to the shaft fragment. For antegrade intramedullary pinning, two to three K-wires were inserted from the fifth metacarpal base, passing through the medullary canal, and finally passed the fracture site and the distal tip of the K-wire advanced to the head beneath the subchondral area. For retrograde intramedullary nailing, K-wire was introduced through the metacarpal head in the retrograde direction and advanced proximal shaft. After the K-wire emerged from the fifth metacarpal bone, the proximal end of K-wires was further pulled out until the distal ends of K-wire was cleared from the end of the articular surface of the head.
2. Measurement of fracture profile
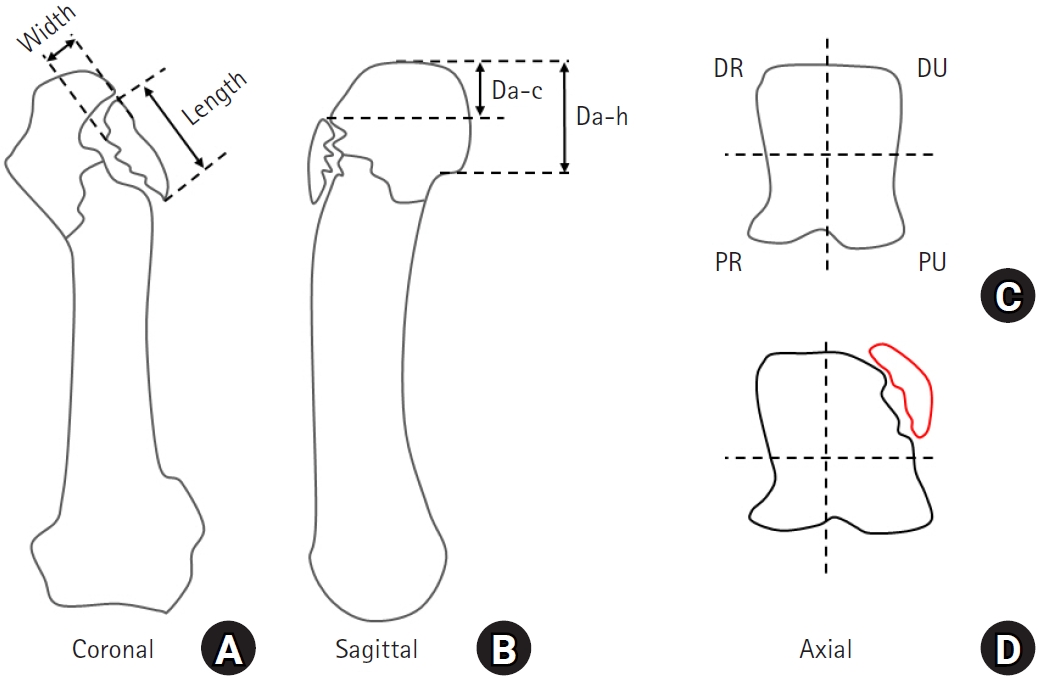
Preoperative CT scans were used to measure the profile of fracture fragments. When the comminution of the fifth metacarpal neck fracture was identified on the CT scan, the length and width of the comminuted fragment were measured on the coronal view of the CT scan (Fig. 1A). The distance from the articular surface of the fifth metacarpal head to the comminuted fragment (Da-c) and the distance from the articular surface to the proximal end of the metacarpal head (Da-h) were measured on the sagittal view of the CT scan to analyze the length and ratio of the intact portion of the metacarpal head cortex (Fig. 1B). To allocate the location of the fracture fragment, the axial cut of the CT scan at the fracture was divided into four quadrants. Four quadrants were classified as dorsal-ulnar (DU), dorsal-radial (DR), palmar-radial, and palmar-ulnar (Fig. 1C). If the fragment involved more than one quadrant, the quadrant of the dominant portion of the fragment was allocated (Fig. 1D).
3. Statistical analysis
Continuous variables were presented as mean with standard deviation, and categorical variables were presented as frequencies with proportion. The length and width of the fragment, Da-c, and Da-h were independently assessed twice by two orthopedic surgeons (DK and SMS.). Intraobserver and interobserver agreements were determined using intraclass correlation coefficients (ICCs). A guideline [17] for evaluating ICCs values was adopted: excellent (>0.90), good (0.75–0.90), moderate (0.50–0.75), and poor (<0.50). All statistical analyses were performed using Python programming language (Python Foundation; https://www.python.org).
Results
1. Patients’ demographics
A total of 113 patients diagnosed with a fifth metacarpal neck fracture were potentially enrolled. After excluding 72 patients according to the exclusion criteria, 41 patients were finally included in this study. The mean age of the included patients was 39.7±13.9 years old, and 40 patients (97.6%) were male (Table 1). In the mechanism of trauma, direct blow accounted for the majority (53.7%), followed by falls (31.7%) and traffic accidents (14.6%). Among 41 patients with fifth metacarpal neck fractures, comminuted fracture fragments were observed in 35 cases (85.4%). All patients underwent surgical treatment according to the surgical indication; retrograde cross pinning and antegrade intramedullary pinning were the dominant techniques performed in 18 (43.9%) and 16 (39.0%), respectively.
2. Fracture profile of comminuted fragments
The mean length and width of comminuted fracture fragments were 7.5±2.3 and 3.2±0.8 mm, respectively (Table 2). The comminuted fragments were on the dorsal aspect of the fracture in all cases, 27 (77.1%) in the DU quadrant and 8 (22.9%) in the DR quadrant. The mean Da-c and Da-h were 5.3±1.6 and 10.9±1.5 mm. The ratio of Da-c to Da-h was 0.5±0.1.
3. Intraobserver reliability and interobserver agreement assessment
The intraobserver reliability of the first rater was excellent for the length, width, Da-c, and Da-h. That of the second rater was excellent for the length and Da-c, good for the width and Da-h. The interobserver agreement between raters was excellent for the length (ICC, 0.987; 95% confidence interval [CI], 0.97–0.99), width (ICC, 0.906; 95% CI, 0.82–0.95), Da-c (ICC, 0.970; 95% CI, 0.94–0.98), and Da-h (ICC, 0.974; 95% CI, 0.95–0.99).
Discussion
This study demonstrates that the fragments of all comminuted fifth metacarpal neck fractures were identified in the dorsal aspect, especially in the DU quadrant. This finding indicates that if the K-wires go to the DU quadrant, the stability of the distal fragment is in danger.
In our cases, most of the fifth metacarpal neck fractures were treated through retrograde crossed pinning (43.6%) or antegrade intramedullary pinning (39.0%). Various surgical methods have been suggested for the fifth metacarpal neck fractures. Plate fixation is rarely indicated due to the problems of tendon adhesion, scar formation, joint stiffness, and issues associated with surrounding soft tissues [18,19]. The retrograde crossed pinning or retrograde intramedullary nailing is an easy and familiar technique, but earlier results showed inferior results in the range of motion and pain than the antegrade intramedullary pinning technique due to the potential risk of tendon injury, joint irritation, and consequent difficulty in the start of early range of motion exercise [16]. Furthermore, rigid fixation across the fracture site in retrograde cross pinning or nailing is sometimes difficult when the distal fragment is small or fracture comminution is severe [10].
To obtain stable fixation, both proximal and distal fragments of the fifth metacarpal neck fracture should be securely fixed by the K-wires both in retrograde cross pinning or antegrade intramedullary pinning. Especially, when there is comminution around the fracture site and the distal fragment is small, the position of K-wires in the distal fragment is critical for stability. Recently, the multiple intramedullary K-wire pinning technique (Bouquet technique) for the fifth metacarpal neck fracture is getting increased popularity for its convenience and minimal invasiveness [20,21]. In the intramedullary pinning for the metacarpal neck fracture, stable three-point fixation increases the stability of the construct and prevents migration of the K-wires [22]. During the procedure, the bent tip of the K-wire that passed across the fracture site usually be pointed dorsally. However, our study revealed that most of the comminuted fragments of the fifth metacarpal neck fracture were located on the dorsal aspect, especially in the DU quadrant. If the bent distal tip of the K-wire is carelessly pointed to the dorsal side, it will be usually directed to the area of the comminuted fragment, which may result in an unstable construct without obtaining a solid three-point fixation (Fig. 2A). We recommend that just after the K-wire passes the fracture site, a rigid three-point fixation will be obtained by rotating the K-wire and pointing the bent tip toward the palmar-radial quadrant of the head where more bone mass presents (Fig. 2B).
This study also revealed that the intact portion in the dorsal aspect of the head (Da-c) is shorter than the length of the comminuted fragment (5.3 mm vs. 7.5 mm, respectively). Furthermore, the intact, non-comminuted dorsal portion of the metacarpal head was only observed in the distal 50% of the metacarpal head size. In other words, when there is a comminuted fracture of the fifth metacarpal neck, it is difficult to secure stable fixation of the K-wire across the fracture site due to the limited intact portion in the dorsal aspect of the metacarpal head. Therefore, before surgery, the intact dorsal portion should be accurately assessed using CT scans, and the degree of K-wire bending should be adjusted to ensure the K-wire proceeds through the intact dorsal portion of metacarpal head. If it is still challenging to direct the K-wire through the dorsal intact portion of metacarpal head, the surgeon may consider directing the K-wire towards the palmar side to achieve stable fixation, necessitating thorough preoperative planning.
The reason for the frequent comminution at the dorsal aspects of the metacarpal neck fracture is not yet clear. The first consideration is the effect of interosseous muscles around the fifth metacarpal bone. A boxer’s fracture is typically a result of direct trauma to a clenched fist where energy is transferred through the fifth metacarpal axially and mostly results in apex dorsal angulation due to the pull of the interosseous muscles of the hand [23]. In the process of dorsal angulation, the dorsal cortex is thinner than the volar cortex making comminution at the dorsal side. Secondly, the metacarpal neck is surrounded by extensors, flexor tendons, and muscles of the interossei, lumbrical, and hypothenar musculature. However, the DU aspect of the fifth metacarpal neck and the head is a bare area without soft tissue coverage except for overlying skin (Fig. 3).
This study has several limitations. Firstly, the study design was case series that can be prone to selection bias, as only patients with the fifth metacarpal neck fractures who underwent CT scans were included in the study. This may lead to bias in which patients with severe comminution or those who received surgical treatment are predominantly enrolled. Nevertheless, we tried to clarify the study objectives and follow a defined study protocol [24]. Secondly, the study was unable to report clinical outcomes such as postoperative functional scores and complication rates. Future research is needed to analyze the correlation between the fracture characteristics of fifth metacarpal neck fractures and clinical outcomes. Thirdly, the cut of CT scans for measurement of fracture profile was not standardized and might vary according to the angulation of the fracture site. However, we tried to obtain standardized data as much as possible by setting a constant reference and repeated measurements. Fourthly, we evaluated the fracture profile with the length and width of a comminuted fragment, which does not sufficiently reflect the three-dimensional nature of the fracture fragments. Further biomechanical analysis using a finite element modeling or cadaveric fracture model may be needed.
Conclusion
Comminutions of fifth metacarpal neck fractures were mainly identified in the dorsal aspect, especially the DU quadrant. To ensure stable K-wire fixation, it is essential to obtain a preoperative CT scan to identify the location and characteristics of the comminuted fracture fragments and subsequently choose an appropriate K-wire position and surgical method accordingly.