Circumferential resurfacing using the bilateral hypothenar free flaps in a patient with finger squamous cell carcinoma patient: a case report
Article information

Abstract
Soft tissue reconstruction of a circumferentially degloved finger is a major challenge. A 64-year-old male patient with underlying diabetes and hypertension presented with biopsy-proven squamous cell carcinoma involving his entire finger. The entirety of his finger was circumferentially degloved to obtain a safety margin. The finger was reconstructed using bilateral free hypothenar flap, and the patient recovered without any complications.
Introduction
To reconstruct digital phalanx soft tissue defect, there are various options including reverse digital artery island flap, thenar flap, hypothenar free flap, toe pulp flap, and venous free flap [1]. A sensate hypothenar free flap is a good tool to reconstruct skin defects with good sensory recovery [1]. However, the flap size is not sufficient to resurface a circumferentially degloved finger. We present a case where the patient’s entire index finger was degloved to excise the squamous cell carcinoma and soft tissue coverage was done by circumferential wrapping using a bilateral free hypothenar flap. To our knowledge, this is the first case where two free hypothenar flaps were used to cover an entirely degloved finger.
Case report
This study was approved beforehand by the Institutional Review Board of Seoul National University Bundang Hospital (No. B-2212-798-701) and performed in accordance with the principles of the Declaration of Helsinki. Written informed consent for publication of the clinical images was obtained from the patient.
A 68-year-old male patient with underlying diabetes mellitus type presented with a skin lesion on his right finger. Punch biopsy done at dermatology department showed Bowen disease. The patient received eCO2 laser and Aldara cream. Ten years later, the size of the lesion increased up to the point of encompassing the entire index finger as shown in Fig. 1 and the patient was referred to our department. Keratosis was observed and the patient complained of no symptoms other than itching sense. The most recent punch biopsy showed squamous cell carcinoma. Preoperative chest and abdominopelvic computed tomography showed no evidence of distant metastasis. Hand magnetic resonance imaging showed diffuse enhancing thickening limited to dermal subcutaneous layer of the right 2nd finger from distal to the middle phalanx. No bone invasion was observed.
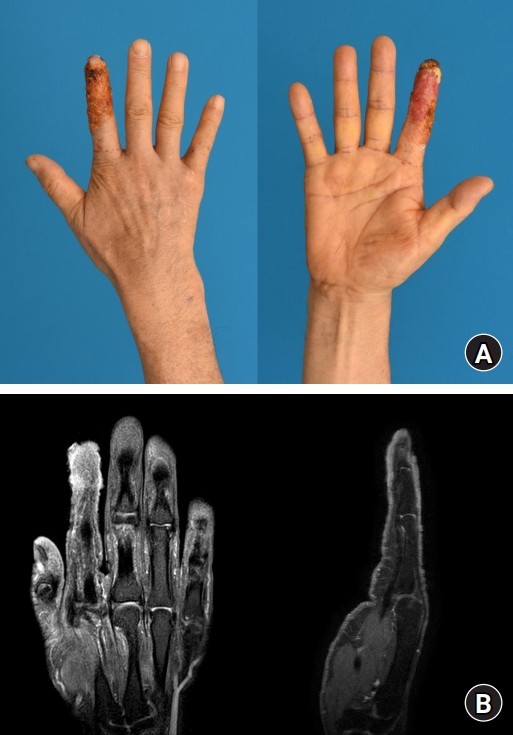
(A) Preoperative photographs showing squamous cell carcinoma encompassing the entire right index finger from the distal phalanx to the mid-phalanx level. (B) The magnetic resonance imaging shows diffuse enhancing of thickening of dermal and subcutaneous layer at 2nd finger middle to distal phalanx without evidence of bone invasion.
Wide excision was planned by degloving the entire finger with preservation of tendon, ligaments as shown in Fig. 2. The extensor and flexor tendon sheaths were removed to ensure complete removal of the tumor. Neurovascular bundles were ligated at the mid proximal phalanx level. The involved finger was totally delgoved with a proximal safety margin of 1 cm. The safety margin was confirmed by intraoperative frozen biopsy.

Photographs of the degloved right index finger after wide excision of the skin lesion.
Skin circumferential resurfacing was done using bilateral free hypothenar flap as shown in Fig. 3. Ipsilateral free hypothenar flap with a 6×3.5-cm skin paddle was harvested. The ulnar artery perforator was anastomosed to the distal end of the ulnar side digital artery in an end-to-end fashion, one cutaneous vein was anastomosed to the dorsal digital vein in an end-to-end fashion. The thickest nerve among the cutaneous nerves arising from the ulnar nerve was harvested together and anastomosed to the digital ulnar nerve. The second hypothenar free flap with the same size was harvested from the contralateral side and vessel anastomosed to the radial side digital artery and dorsal vein concomitantly. Flaps were harvested by a technique described by Kodaira and Fukumoto [1]. Histopathologic examination of the amputation specimen demonstrated a squamous cell carcinoma with a tumor thickness of 2 mm. The investigation confirmed an R0 resection with 0.1-cm proximal safety margin and 0.2-cm deep safety margin. Tumor stage and grading were pT3cN0cM0, G2, and stage III. The patient was discharged 8 days postoperatively and no adjuvant chemotherapy or radiation was administered. For the 20 months of follow-up periods, the patient is very satisfied with the result and showed no difficulty in hand pinch and daily activity as shown in (Fig. 4).

Immediate postoperative photograph showing circumferential finger resurfacing using two free hypothenar flaps.
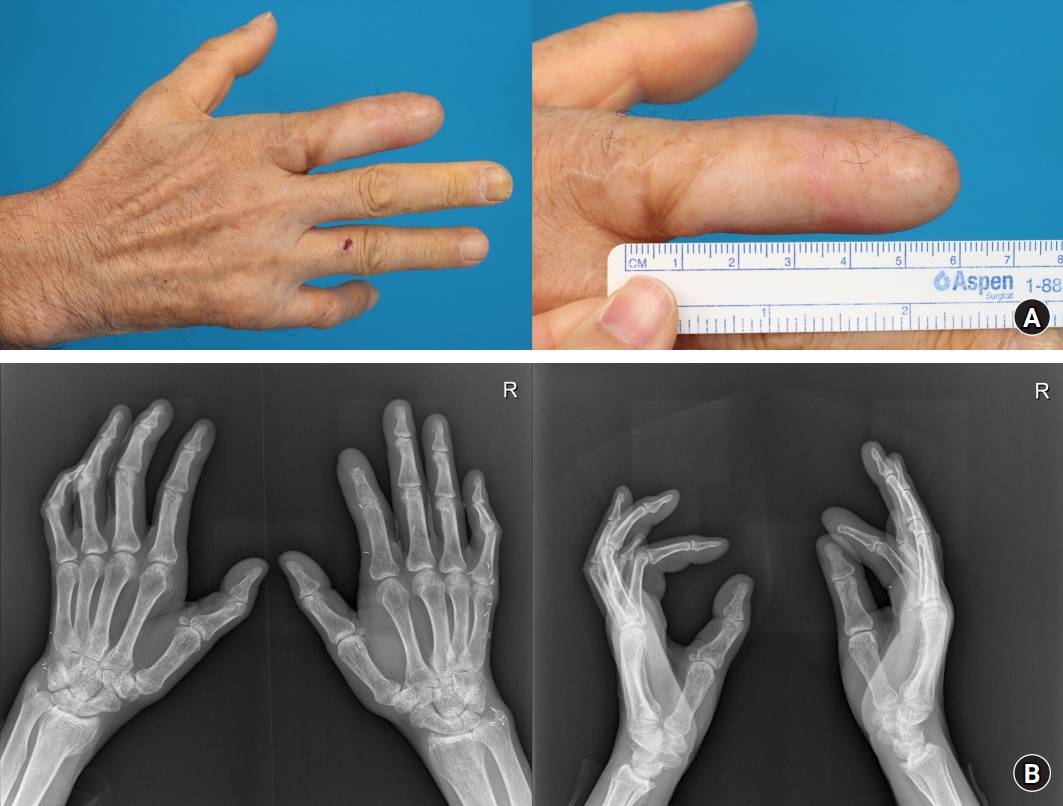
Postoperative 20-month photographs (A) and X-rays (B).
The distal phalanx of the right 2nd finger was observed to be continuously absorbed during follow-up, which appears to have occurred using bilateral digital arteries as recipients during surgery. Currently, the flap is stable, and the patient does not complain of any discomfort in daily life. The middle phalanx bone was observed intact, confirming that the viability of the bone to at least the middle phalanx was guaranteed even if both bilateral digital arteries were used at the proximal level of the proximal phalanx (Fig. 4).
Discussion
Reconstruction of finger defects can be achieved using various flaps. For small defects, an anterograde digital artery island flap can be used. For medium-sized defects larger than half the finger pulp, reverse digital artery island flap, toe pulp flap, and hypothenar free flaps are options. Although reverse digital artery island flap harvest is tedious, donor site closure often requires skin graft coverage. Thenar flap harvest is also tedious but often causes finger joint flexion contracture. Hypothenar free flap harvest requires more care than the aforementioned flap, but the donor site can be closed primarily with a relatively inconspicuous scar [1].
Soft tissue coverage of circumferential degloved finger is a great challenge. Skin grafts cannot be used due to contracture, non-gliding tendons, and avascular necrosis of distal bones [2]. Flaps are required to cover exposed tendons, ligaments, joint capsules, and neurovascular bundles [2]. Reconstruction should provide a pliable and sensate skin without hindering motor function [3,4]. Local flaps near the hand that match the texture of the finger may be used but they are limited by the flap size and defect location [5]. For example, a reverse dorsal digital island flap may be used, but the flap size is not sufficient to cover an entire phalanx [6]. Distant pedicled flaps may be used but it requires at least 2 week period where the defect is attached to a distant part of the body which may lead to joint stiffness [7,8]. Free flaps can be used for their versatility in size, shape, and positioning [2]. For degloved digits, the flap should be thin, pliable, yet broad enough to cover the entire digit. Large flaps such as free abdominal, radial forearm free flap, dorsalis pedis flap, anterolateral thigh flap, thoracodorsal artery flap, lateral arm flap, and medial sural artery flap can be utilized, but results in poor cosmetic and functional outcome. They also result in cosmetically unacceptable donor site scars. A great toe wrap around flap can be used specifically for thumb reconstruction but is not suitable for the remaining phalanx [9,10].
The advantage of using free hypothenar free includes excellent skin thickness, color and texture, and pliability of finger. Functional and cosmetic appearance are relatively good [1]. The hypothenar area skin is also unique in that it consists of both dorsal and palmar side skin of the hand. Thus, the dorsal part of the hypothenar skin can be used to reconstruct the dorsal part of the finger and the palmar side of the hypothenar skin can be oriented to cover the palmar side of the finger. The palmar skin of the fingertip is important in sensory function [10]. Thus, using palmar skin for reconstruction of palmar skin is ideal. Harvesting as a sensate flap shows excellent sensory recovery [10]. The great challenge of using hypothenar free flap in resurfacing a circumferential degloved finger is that flap volume is only sufficient to cover semi-circumferentially. In our case, this was overcome by using two flaps to cover the radial and ulnar side each.
There are also disadvantages of hypothenar flap including difficult pedicle dissection. Temporary congestion can be observed, which can be alleviated using bleeding or medical leeches. Due to the bulkiness of flap, additional skin graft may be required to cover the raw surface to avoid pedicle compression [10]. However, these disadvantages are outweighed by the advantages of hypothenar flaps in finger soft tissue reconstruction.
In conclusion, reconstruction of a degloved finger due to trauma or wide excision of skin cancer as in this case is a great challenge. Reconstruction requires abundant soft tissue that also matches the color, texture, and thickness of both the volar and dorsal sides of the original finger skin. Using free hypothenar flap qualifies these qualities in that it consists of both the dorsal and volar sides of the hand. The limited amount of soft tissue to cover an entire finger can be overcome by using two flaps from both hands as in this case. Thus, using bilateral free hypothenar flap is an excellent choice in resurfacing an entirely delgoved finger.
Notes
The authors have nothing to disclose.
Funding
None.