Correction of hand deformities after burns
Article information

Abstract
Hand burns can lead to deformities even after successful primary healing. They are the most common cause of skin contracture involving the hand. This review article discusses ways to correct claw deformity, flexion contracture in the palm and finger, and web space contracture, which are post-burn hand deformities commonly encountered in clinical practice. Loss of skin is the end result in many cases of hand deformities after burns. Therefore, reinforcing the lost skin is the principle of corrective surgery. Even if the skin is thicker than the full-thickness skin, it will engraft if damage to the tissue and blood vessels of the recipient is minimized. The thicker the skin, the less re-contraction and growth occur. The foot is an ideal donor site for skin grafts on the hand. In particular, the instep or the area below the malleolar is a very good donor site. The first web space of the hand is very important for hand function, and it must be reconstructed with Z-plasty, a skin graft, and a free flap step by step according to the degree of contraction.
Introduction
Even if the primary healing is successful, deformity of the hand following burns is the most common cause of skin contracture involving the hand. Whitson and Allen [1] summarized the factors that contribute to hand deformities including persistent edema, wound infection, poor positioning, prolonged immobilization, and delayed or inadequate skin coverage. The incidence of hypertrophic scarring is significantly greater in burns that fail to heal within 3 weeks [2].
MCauley [3] classified burn scar contractures into four grades. Grade I is symptomatic tightness without limitation in range of motion and is characterized by normal architecture. Grade II is mild decrease in range of motion without significant impact on activities of daily living and involves no distortion of normal architecture. Grade III is marked by functional deficit, with early changes in normal architecture of hand. Grade III is subclassified into flexion, extension, and combination contractures. Grade IV entails loss of hand function with significant distraction in normal hand architecture. Donalon [4] classified post-burn hand deformities into three general categories: soft tissue deformities, joint deformities, and amputations because they are highly variable.
The end result leading to hand deformities after burns is mostly loss of skin. In deep second or higher degree burns, secondary contracture of the grafted partial-thickness skin tends to occur eventually even after healing for more than 3 weeks with or without skin graft, resulting in contracture deformation of the hand. Therefore, most of the treatment for contracture deformation after upper extremity burns entails contracture release or removal of scar tissues, followed by skin graft to cover the resulting skin defect. Flap surgery is indicated if important structures such as tendons or nerves are exposed. This review article explains how to correct claw deformity, flexion contracture involving palm and finger, and web space contracture, which are post-burn hand deformities generally encountered in clinical practice.
Claw deformity
Claw deformity involves extensive extension of the metacarpophalangeal (MP) joint and flexion of the interphalangeal joint, and it is one of the most difficult deformities to reconstruct (Fig. 1).

Claw hand deformity after a hand burn. A deformation in which the metacarpophalangeal joint is excessively extended and the interphalangeal joint is flexed is shown.
The movement of the MP joint is preserved and the proximal interphalangeal (PIP) joint is placed in a functional position. Skin defects occur when the contracture is released by approaching the dorsal side of the MP joint first. This defect should be covered with a full-thickness skin graft [5]. Flap surgery should be considered if important structures such as tendons or nerves are exposed (Fig. 2). If necessary, collateral ligament release, capsulotomy, and palmar plate release can be performed together. In particular, claw deformities in children require attention because hyperextension of the MP joint is difficult to correct. Extensive incision of the entire MP joint and reconstruction of the hand dorsum using a free flap are often required [6].

Tangential excision and full-thickness skin graft. If complete flexion of the metacarpophalangeal joint is difficult due to burn scar formation on the back of the hand, complete flexion can be achieved by removing all of the scar tissue, followed by full-thickness skin graft surgery.
Flexion contracture of palm and finger
Surgery to correct flexion contractures of the fingers after burns is one of the most common surgeries performed to correct deformity after burns. Corrective surgery is mandatory since finger flexion contracture limits the entire hand function and not only the fingers (Fig. 3).

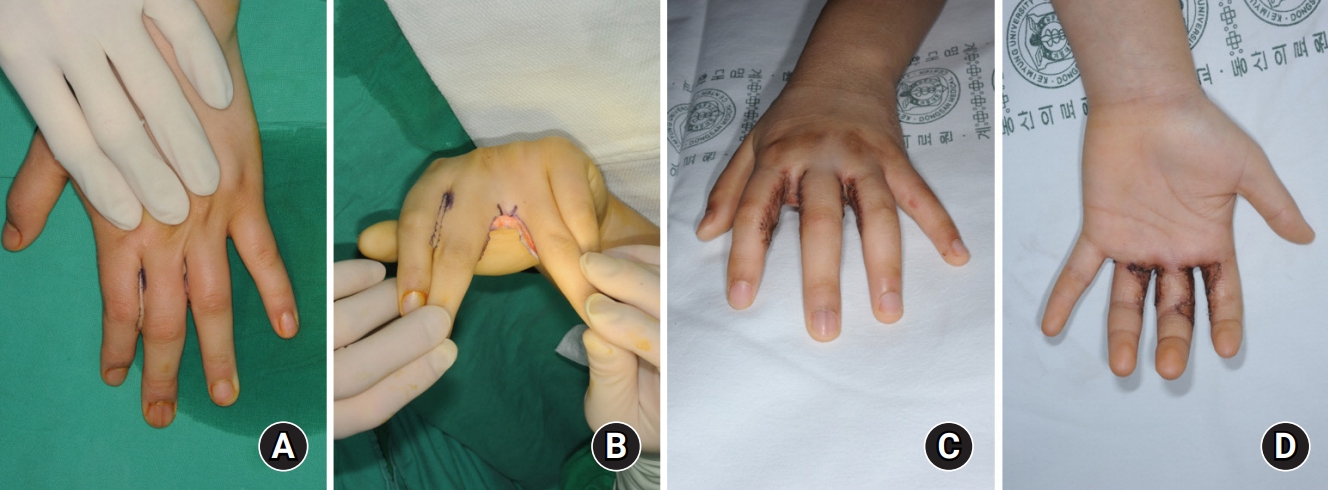
(A, B) A 10-month-old boy who suffered a steam burn from a pressure rice cooker and developed flexion contracture in the palm, long, ring, and little fingers after conservative management. (C, right) The scar tissue was completely removed and a full-thickness skin graft from the groin was performed to correct the flexion contracture. (C, left) Ten days after skin graft.
Kurtzman and Stern [7] classified flexion contractures of the fingers after burns into different types. Type I is a contracture involving only the skin; passive flexion of the MP joint is possible, and the PIP joint can be fully extended. Type II contracture involves the capsular structure of the palm, and passive flexion of the MP joint is possible, but not passive extension of the PIP joint. Type III contracture involves both soft tissue and joint and the PIP joint is fixed regardless of the MP joint position.
In the case of type I, since only the skin is insufficient, an incision is made in the contracted area to sufficiently release the contracture and enable a full-thickness skin graft (Fig. 4). The operation is performed under general anesthesia and a tourniquet, without squeezing the blood completely, but leaving sufficient blood in the vein. A fish-mouse incision in the area with the most severe contraction is followed by insert of the incision up to the dermis with a surgical knife and application of physical force to fully straighten the finger to preserve the para-tendon without injuring nerves or blood vessels. The scar tissue or band found in this process is sharply removed or cut with a tenotomy scissors. After releasing the tourniquet, the bleeding point should be accurately found by irrigation with normal saline, followed by hemostasis via bipolar electrocautery to minimize tissue damage.
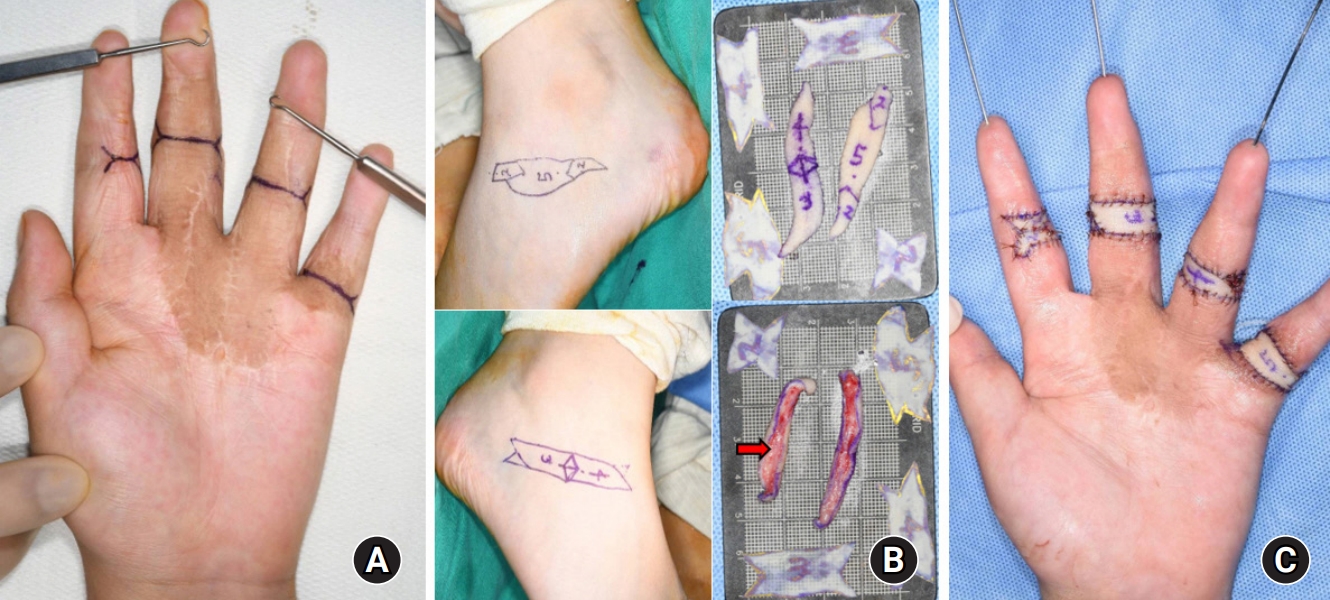
(A) The flexion contracture recurred in the same boy as described in Fig. 3, at the age of 10 years. (B, C) After contracture release via a fish-mouth incision, a full-thickness skin with partial subcutaneous fat (red arrow) from both inferior malleolar areas was grafted and the fingers were immobilized with Kirschner wires.
In general, a full-thickness skin graft means that the skin is harvested, including subcutaneous fat, and then the fat is completely removed and grafted. This is because the subcutaneous fat layer is known to interfere with inosculation, the process of microvascular connection required for skin engraftment. The author’s previous study found that the subcutaneous fat layer did not act as a barrier but rather functioned as a source of vessel communication [8]. Based on the author’s research and clinical experience, the author would like to emphasize that the following principles must be followed to successfully engraft composite skin, which is full-thickness skin containing fat. The first principle is to properly prepare the recipient’s wound bed. This is to minimize tissue damage and preserve the microvessels as much as possible. The second is to thoroughly maintain contact between the recipient bed and the composite skin. This is to prevent a hematoma after skin grafting and apply a compressive dressing such as a bolus dressing. The third is to remove the risk factors during the composite skin graft process by immobilization with Kirschner wire and prevent swelling by hand elevation [9-11]. It takes 2 to 3 weeks for thick composite skin to completely engraft, and subsequent wearing of a dynamic splint prevents secondary contracture of the transplanted skin. The thicker the skin, the less is the need for re-contraction and growth.
Many surgeons select groin as a full-thickness skin graft, which facilitates harvesting of large skin, but posttransplantation pigmentation is a drawback. However, the color match with the palm is good when the skin is obtained from the inner or outer inframalleolar or medial plantar of the foot (Fig. 5) [12].

(A, left) An 11-year-old boy, who sustained a burn at 1 year of age and was treated with a full-thickness skin graft from the groin, shows residual pigmentation (black arrows). (A, middle and right) On day 9 after the full-thickness skin graft with a part of subcutaneous fat from both inferior medial malleolar areas after complete release of the flexion contracture. (B, left) Wearing a dynamic splint. (B, middle) The color match of the grafted skin (red arrows) is excellent 3 years after surgery.
In the case of type II, it is often necessary to release the volar plate and separate the checkrein deformity to release the stiff joint. In this case, since the joint capsule is exposed and the flexor muscle is exposed, it must be covered with a flap. For type III, joint fixation is preferable.
If the width of the burn scar is narrow and forms a band, the scar can be excised and corrected simply with multiple Z-plasty or double-opposing Z-plasty (Fig. 6).

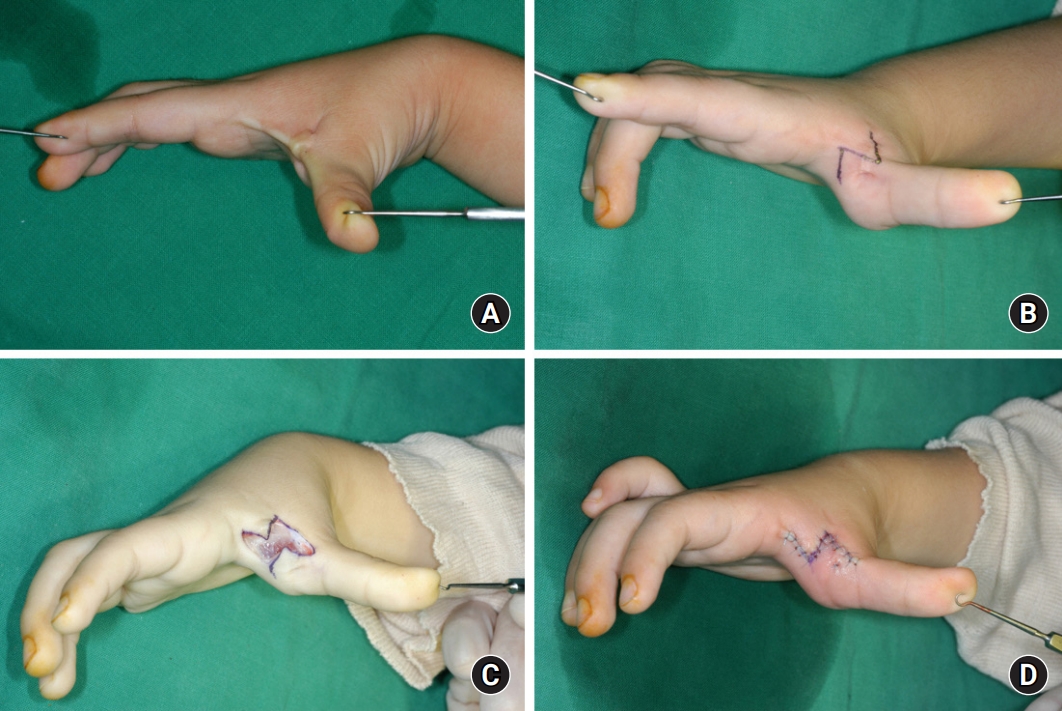
(A) The flexion contracture caused by a narrow and long scar on the volar side of the thumb was corrected with multiple Z-plasty. (B) After flap transposition.
Palmar contracture can occur when a child or person with epilepsy grabs a hot object [13]. In a country where rice is the staple food, when a steam burn is caused by the steam outlet of a pressure electric rice cooker, the burns are deep and contracture involves the fingers, including the palms, when they are healed without skin graft. In case of burn scar adhesion or flexion contraction of the fingers including the palm, the scar is completely excised, the contracture is sufficiently released, and a full-thickness skin graft is performed (Fig. 3).
Web space syndactyly/interdigital contracture
Syndactyly of adjacent fingers after burns is caused by fusion between burned fingers during healing or movement of the web distally due to flexion contracture of fingers (Figs. 7, 8). Corrective surgery is based on Z-plasty and various modifications of Z-plasty (double-opposing, four-flap, five-flap [V-M], and VYZZ plasty) are performed (Figs. 9, 10) [14]. However, since Z-plasty cannot sufficiently compensate for insufficient skin in many cases, a full-thickness skin graft is often required simultaneously, and flap surgery is required when important structures are exposed [15,16] (Fig. 11). Recontracture may occur if skin graft is not performed sufficiently, and even if the graft is adequate, a recurrence of syndactyly may be reported.
(A) Syndactyly developed due to adhesion of the adjacent fingers after a burn. (B) Recurrence can be prevented by completely removing the scar tissue, securing enough interdigital web space with a releasing incision, (C, D) followed by grafting of sufficient full-thickness skin.

(A) Syndactyly in a 6-year-old boy, who was exposed to a steam burn at 10 months of age. Syndactyly occurred as the web space moved distally due to flexion contracture of the fingers. The first operation on this patient was a skin graft for contracture at 7 months of age. (A, middle) During a second operation, flexion contracture and web space were released and a full-thickness skin graft was performed. (A, right) The photograph was taken 6 months after the operation, and the syndactyly was completely corrected. (B, left and middle) Syndactyly recurred at the age of 15 years, and the same operation was performed a third time. (B, right) At the age of 22 years, syndactyly recurred, and the fourth and final corrective surgeries were performed.
(A) A contracting band and scar tissue in the first web space are noted. (B) Design of single large Z-plasty. (C) Complete excision of the contracting band and scar tissue before transferring the triangular flaps to each other. (D) After flap transposition.

(A) Design of double-opposing Z-plasty in the first web space. (B) After flap transposition.

(A,B) In order to create the first and second web space, an incision was made on the contracture, followed by sufficient web space and a full-thickness skin graft. A Kirschner wire is very useful not only for immobilization and securing space, but also for engraftment of thick skin. (C) The web spaces were well maintained.
Adduction contracture of the first web space is an adduction contracture of the thumb due to fibrosis of the adductor muscle or first dorsal interosseous and is distinct from the aforementioned web space contracture [17]. Web space contracture is confined to the skin, whereas adduction contracture is accompanied by muscle fibrosis. Choi et al. [18] classified the first web space contracture into mild, moderate, and severe types, warranting reconstructive surgery. Mild contracture is confined to the skin and deep fascia is not damaged. It is corrected with Z-plasty, modified Z-plasty, and Z-plasty augmented with grafting. Moderate contracture entails damage not only to the skin but also to the deep fascia. In case of thick scar tissue and fibrous fascia, an incision in the muscle may be required to widen the web space sufficiently, followed by reconstruction with a skin graft or flap (Fig. 12). Severe contracture is accompanied by fibrosis of the muscles constituting the first web space and deformation of the joints of the thumb and index. The metacarpal bone of the thumb undergoes adduction and supination, and the MP joint compensates for excessive extension and abduction due to pseudoabduction of the thumb to grasp the object. Reconstructive surgery can be used to completely remove the scars, release the adductor muscle and the first dorsal interosseous muscle from the origin to ensure a well-spread first web space and reconstruct with a free flap. The foot-first web space free flap is very useful as a donor site for hand-first web space reconstruction but is associated with donor site scars. However, this disadvantage can be prevented to some extent using a full-thickness skin graft including the subcutaneous fat layer or artificial dermis (Fig. 13). Other useful free flaps include lateral arm, dorsalis pedis, and anterolateral thigh-free flap (Fig. 14).
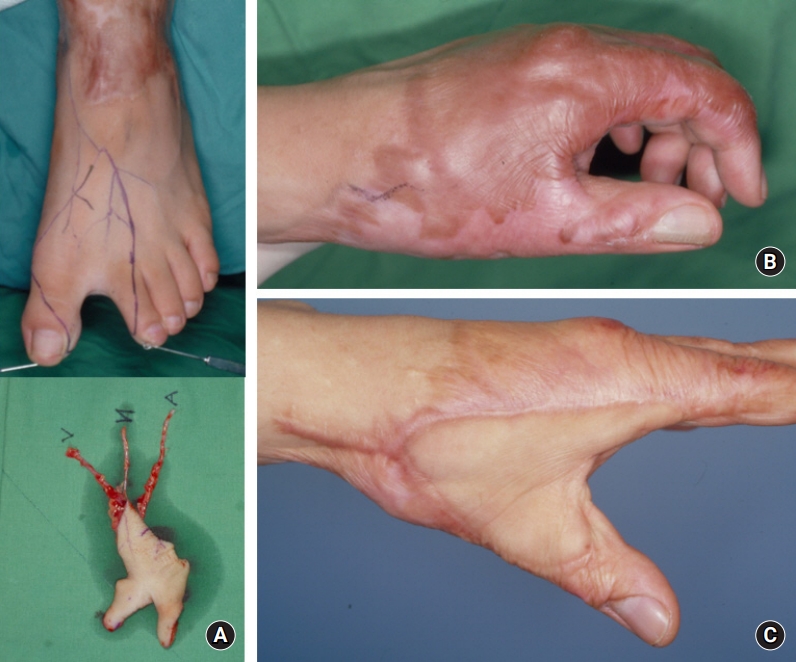
(A) Design of a foot-first web space free flap is shown. (B) A hypertrophic scar is covered on the dorsum of the hand, including the first web space, which prevents full abduction of the thumb. (C) Appearance after reconstructive surgery.

(A) A 23-year-old female patient had severe adduction contracture in the first web space after suffering a flame burn 18 months previously. (B) Release of the adductor and first dorsal interosseous muscles (red arrows) was followed by correction of adduction and supination of the metacarpal bone of the thumb and compensatory hyperextension of the metacarpophalangeal joint. (C) Reconstruction was followed by covering the defect with dorsalis pedis free flap.

(A) The palm and first web space were damaged by the inlet of a high-voltage electric burn. (B) The toes were in contact with an electrical outlet. (C) The palm defect including the first web space was reconstructed with an anterolateral thigh free flap.
All clinical figures used in this review are those of patients treated by the author. Written informed consent was obtained for publication of those images.
Conclusions
Hand deformities after burns complicate the patient’s daily life and interfere with daily social life. Even with very severe deformities, the hand surgeon should focus on the functional aspects of the hand and perform reconstructive surgery with a very functional hand. The technique can be used to completely engraft the full-thickness skin graft including a part of the subcutaneous fat layer. Based on the fundamental principles of hand surgery, the microsurgical technique can be used to transform the hand deformity after a burn into a functional hand.
Notes
The author has nothing to disclose.
Funding
None.