An Epidermoid Cyst along the Sensory Branch of Digital Nerve with Focal Neuropathy: A Case Report
Article information

Abstract
An epidermoid cyst is a slow-growing benign neoplasm that commonly occurs in the hand. Herein, we report a rare case of an epidermoid cyst with focal neuropathy in the left ring finger of a 38-year-old woman. Preoperatively, the patient complained of erythema, swelling, and paresthesia on her fingertips. On ultrasonography and magnetic resonance imaging, ulnar digital nerve thickening and inflammation around the nerve were observed, and a neurogenic tumor-like schwannoma was expected. An excisional biopsy with neurectomy of the involved sensory branch of the ulnar digital nerve was performed under brachial plexus block. During the operation, there is such an uncommon morphology, yellowish debris under the epineurium of the ulnar digital nerve sensory branch was involved with the epidermoid cyst and seemed to be propagating along the sensory branch from the skin surface. After the operation, the paresthesia and swelling resolved. Over the 6-month follow-up in the outpatient clinic, no complications and recurrences occurred. Thus, we reported a rare intraneural epidermoid cyst (occurred along the digital nerve) in the finger, and we believe that considering the anatomical characteristics and the surrounding structures is important during mass excision.
INTRODUCTION
An epidermoid cyst is a slow-growing benign neoplasm that commonly occurs in the hand [1]. It is caused by the proliferation of the epithelium after inversion under the dermis [2]. Various mechanisms are responsible for the development of epidermoid cysts, of which the most common are related to previous trauma and human papillomavirus infection [3]. All body lesions can develop into an erupted epidermoid cyst. However, the finger is composed of various structures in limited spaces, such as a digital neurovascular bundle, tendon, phalangeal bone, and ligaments. Therefore, the mass effect on the finger is greater than that on other large structures, such as the abdomen and upper arm. In addition, if the mass compresses the structures in the finger, it can cause other symptoms related to the compression of the structures. In this article, we report a case of an epidermoid cyst on a finger with an intraneural invasion of the digital nerve.
CASE REPORT
Institutional Review Board of Korea National Institute for Bioethics Policy approved this case report (No. DSMC-2021-05-021, KoNIBP-P01-202109-21-008). A 38-year-old woman visited our hospital because of a left ring finger (LRF) mass lesion with fusiform swelling for 1 month without any trauma history (Fig. 1). Written informed consent was obtained for publication of this case report and accompanying images. Before her visit to our hospital, she visited another orthopedic clinic, where the orthopedic physician recommended close observation because no abnormality was detected on plain hand radiography. Although she waited for 1 month for the LRF mass lesion and pain to resolve with antibiotics and anti-inflammatory agents, these were not resolved. In our clinic, an approximately 1-cm-sized soft mass with redness was found on the P1 volar side. No skin lesions such as ulceration or punctum were found. The patient complained of ulnar side dullness of the left ring fingertip. Tenderness was observed around the mass lesion, and the pain was aggravated during finger extension. In addition, Tinel’s sign was found around the LRF mass lesion, and a tingling sensation spread to the ulnar side of the LRF.

The mass with fusiform swelling, pain, and paresthesia on the volar side of the left ring finger 1 month before treatment.
Plain radiography revealed no bony abnormalities, except for a soft tissue swelling around the P1 area. On ultrasonography, ulnar digital nerve (UDN) thickening and swelling were observed in the LRF, and a neurogenic tumor was expected (Fig. 2). On magnetic resonance imaging, unencapsulated and segmental thickening with surrounding edema was found along the UDN from the metacarpophalangeal joint of the LRF to the proximal interphalangeal joint of the LRF. No bony or joint involvement was observed (Fig. 3).
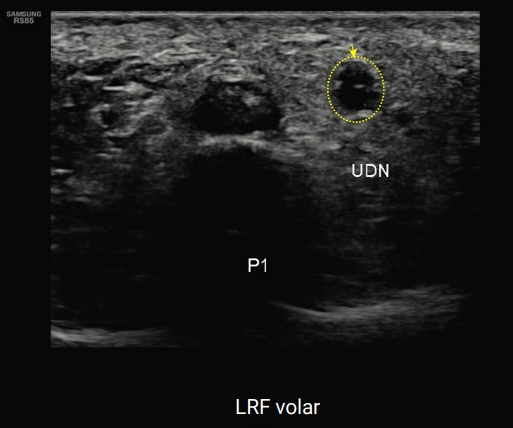
Ultrasonography image showing the swelling and thickening of the ulnar digital nerve (UDN; yellow circle and arrow). A neurogenic tumor was expected. LRF, left ring finger.
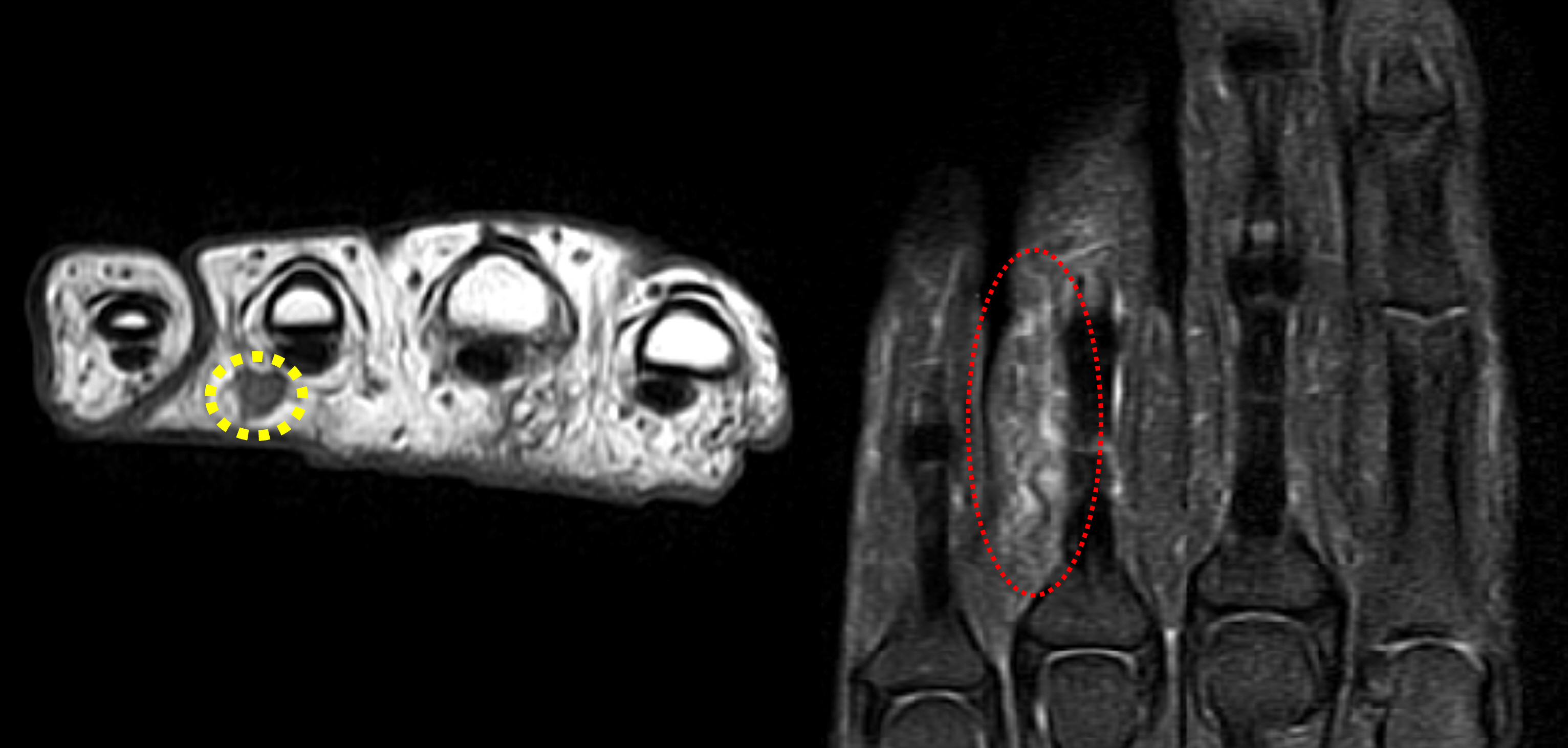
Magnetic resonance image showing unencapsulated and segmental thickening (yellow dotted circle, left) with surrounding edema (red dotted circle, right) along the ulnar digital nerve. A neurogenic tumor was expected.
Before the operation, as we did not expect the presence of a well-defined margin between the digital nerve and mass, we received the consent of the patient that only partial excision would be performed; however, if a malignancy was expected, the mass would be excised together with the digital nerve, followed by reconstruction with a nerve graft.
The patient proceeded with an excisional biopsy. Midlateral incision was made on the LRF proximal phalanx, and swelling with UDN was observed. Around the UDN, small branches toward the skin surfaces were found, and the epidermal cyst contained yellowish debris encircling and involving one branch. In addition, the epidermal cyst was propagating toward the skin, under the epineurium and connected to the main branch of the UDN. Therefore, we excised the total sensory branch with the cyst (Fig. 4).
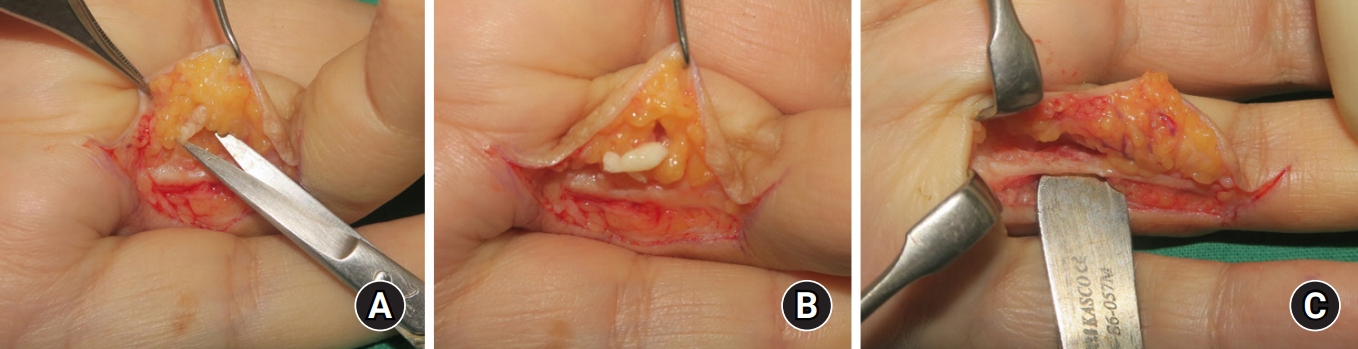
(A) The epidermal cyst containing yellowish debris encircled and involved the sensory branch of the ulnar digital nerve. (B) The epidermal cyst with yellowish debris propagating toward the outer skin. (C) The preserved main branch of the ulnar digital nerve after neurectomy.
Histological examination revealed that the cyst was surrounding the main digital nerve and its branch, with many acute inflammatory cells lined by the true epidermis (inflamed epidermal cyst). No evidence of malignancy was found, and the cyst contained keratin materials (Fig. 5).
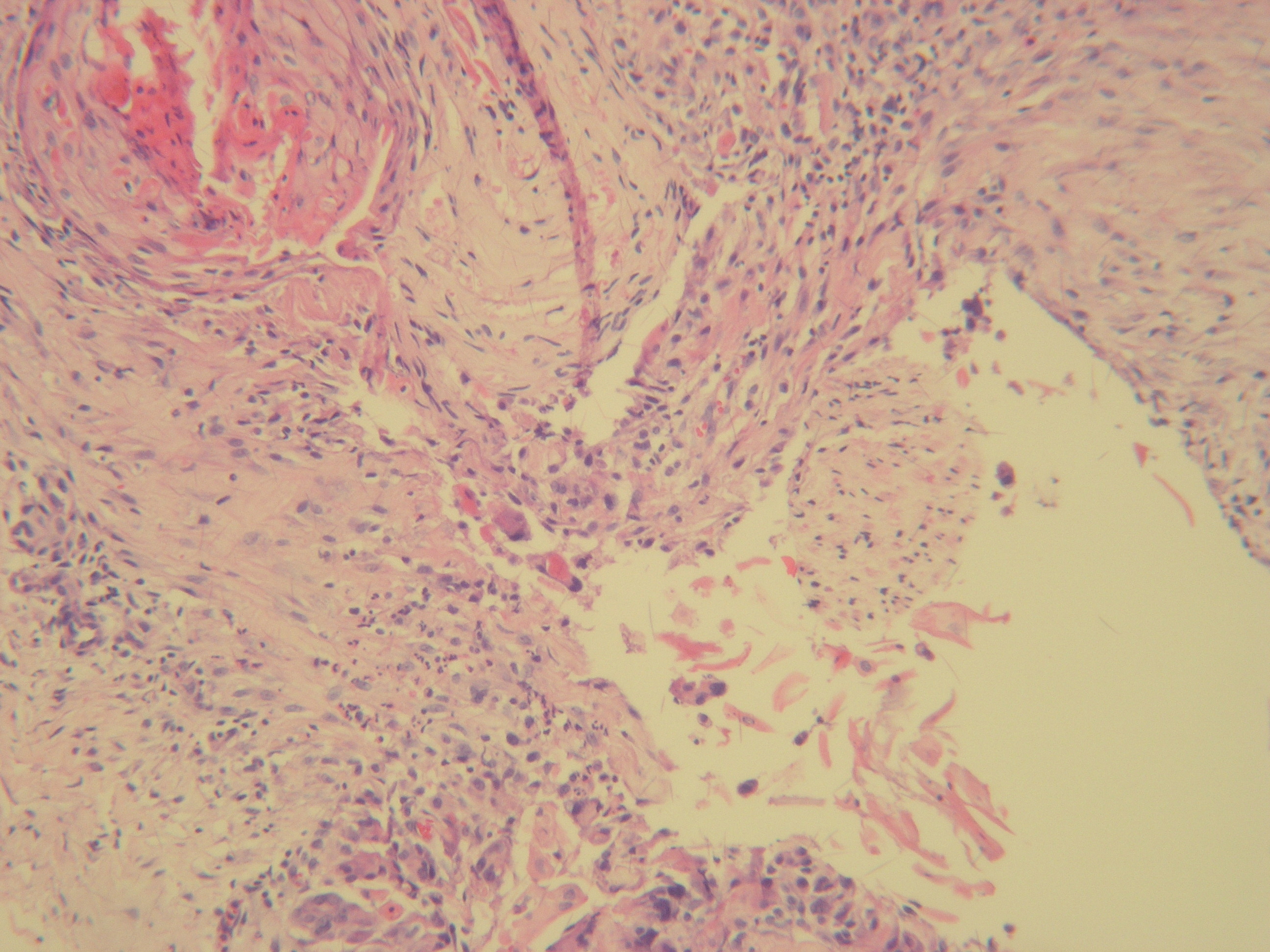
Histological examination showing many acute inflammatory cells lined by true epidermis around the digital nerve (H&E stain, ×100).
The patient’s postoperative course was favorable. No sign of recurrence and infections were observed at the 6-month postoperative follow-up. During the outpatient clinic visits at 1, 3, and 6 months after the operation, follow-up ultrasonography was performed. At 1 month after the operation, digital nerve thickening was observed; however, it resolved 6 months after the operation. The dullness of the fingertip and Tinel’s sign were resolved 6 months after the operation, and no postoperative complications were observed (Fig. 6).

Six months postoperative appearance showing a full range of motion without any complications and symptoms.
DISCUSSION
An epidermoid cyst can erupt anywhere in our body. Various studies have been conducted on the incidence of epidermoid cysts. In the hand and forearm, the incidence of epidermoid cyst ranged from 4.5% to 16% [1,4,5]. Lesions on the dorsum of the hand are closely related to previous trauma history [1]. In our case, the epidermal cyst occurred around the digital nerve and caused focal neuropathy without any trauma history. Although she didn’t remember any trauma on her finger, the volar side of finger is a location where many stimuli occur in daily life; therefore, it is hard to suggest that our case will not be related to trauma. The patient in our case report suggests that the epidermoid cyst may have been caused by an unsuspecting trauma or that an epidermoid cyst that had spread along a skin appendage such as a sweat gland extended to a digital nerve branch. To our knowledge, only two cases of an intraneural epidermal cyst with focal neuropathy have been reported [2,6]
Bohler et al. [2] reported a ruptured epidermal cyst with paresthesia that propagated its extension along the length of the finger. Its symptoms resolved after excision. The cyst was limited to the subcutaneous layer; however, it suggested that the lesion with inflammatory propagation was related to focal neuropathy [2]. In addition, Imai et al. [6] reported a spherical mass wrapped around the radial digital nerve. The mass was also under the epineurium of the digital nerve and directly affected the digital nerve resulting in neuropathy. In our case, it was similar to the previous articles, in that the epidermoid cyst was located closely around the nerve and under the epineurium, and caused focal neuropathies. However, the cyst in our report had a very specific and uncommon location and shape. The cyst in our case resembled a neurilemmoma or intraneural ganglion cyst that encapsulates nerve fascicles under the epineurium [7,8]. Because the epidermoid cyst caused the inversion of the epidermis under the dermis, our case showed that epidermoid cyst propagated from the skin surface to the digital nerve along the small sensory branches, unlike neurilemmoma or intraneural ganglion cyst (Fig. 7).
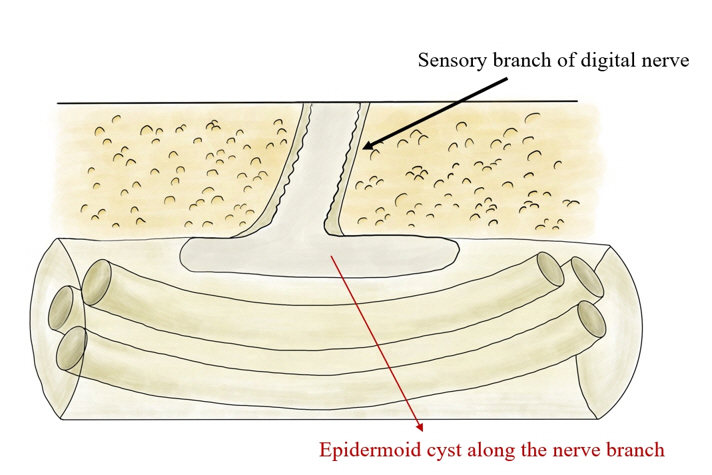
A schematic photograph of the epidermal cyst propagating to the main digital nerve along the sensory branch.
We report a rare case of a patient with focal neuropathy caused by an epidermoid cyst in the hand without a trauma history. After excision of the epidermoid cyst with neurectomy, all the symptoms improved immediately and no complications occurred during the 6-month outpatient follow-up. Fortunately, it was propagated under the epineurium along a small sensory nerve branch of the main nerve; therefore, it was possible to partially resect the nerve with the cyst and preserve the main nerve.
Anatomically, the fingers have multiple structures in limited spaces; therefore, space-occupying lesions of the fingers easily cause focal neuropathy when compared with those in other affordable spaces. Hence, consideration of the anatomical characteristics and surrounding structures during mass excision is important.
Notes
The authors have nothing to disclose.