INTRODUCTION
Soft tissue hand defects require flap coverage to protect exposed structures such as tendons, vessels, and bones as well as to preserve the functioning of the injured hand. Venous congestion, however, can sometimes occur and lead to necrosis of the flap [1]. One procedure to overcome this problem is venous supercharging. In this case report, we discuss our response to a serious degloving injury. One crucial measure we implemented was to apply cephalic vein supercharging to a reverse radial forearm flap to prevent venous congestion. The reverse radial forearm flap is often used for large soft tissue defects on the dorsum of the hand. This flap provides a pliable tissue, a constant blood supply and above all is a technically simple piece of tissue. Thus, by using the reverse radial forearm flap with venous supercharging, we were able to address our patient’s degloving injury and restore his hand to full functioning capacity.
CASE REPORT
A 66-year-old man presented a severe degloving injury on the dorsum of his right hand (Fig. 1). Upon physical examination, there were no fractures, but the 3rd and 4th extensor digitorum tendon were ruptured and the dorsal metacarpal vessels and metacarpophalangeal joint were exposed. Metacarpal bones were also exposed as a result of the injury. After examination, the patient was brought to operation room and the ruptured tendon was repaired after copious irrigation and debridement of devitalized tissue. Following serial debridement combined with antibiotic therapy for 10 days, a coverage procedure was performed on the patient.
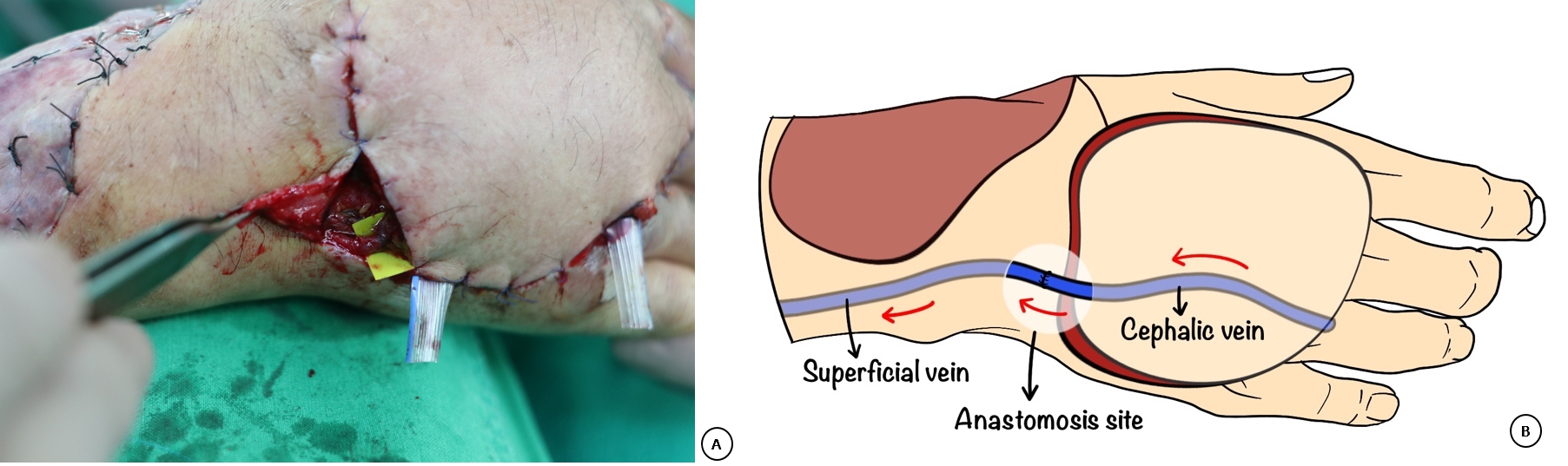
Allen’s test was conducted preoperatively to secure perfusion of the palmar arch by the ulnar artery alone. The remaining defect measured about 9×10 cm with exposure of the extensor digitorum tendon and metacarpal bone (Fig. 2). The course of the radial artery was determined using Doppler (Fig. 3). After tracing the radial artery and the cephalic vein, flap elevation, including the proximal cephalic vein, was performed. During dissection, a superficial branch of the radial artery was ligated and a superficial radial nerve was preserved (Fig. 4). The flap was rotated 180° on the bifurcated site of the deep palmar arch to cover the defect. To prevent postoperative congestion, an additional incision was made on the dorsal side of the hand to identify and dissect a cutaneous vein. Supercharging between the cephalic vein and the superficial vein on the dorsum of the hand was performed with 9-0 nylon (Fig. 5). The donor site for the flap was covered with a split-thickness skin graft (Fig. 6).
The soft tissue defect on the dorsum of the right hand was successfully repaired. The patient recovered well without complications except for a bulky flap covering the defect and a somewhat limited range of motion in 3 to 5 digits. Six months postoperatively, the patient had additional flap debulking surgery and tenolysis (Fig. 7). After 1 year, he could perform most hand functions without inconvenience.
Written informed consent was obtained for publication of this case report and accompanying images.
DISCUSSION
The dorsum of the hand has very thin and fragile skin with little soft tissue. It protects structures such as the extensor tendons as well as metacarpal bones and vessels in the dorsal hand area. Soft tissue defects in the dorsum of the hand commonly occur via trauma, infection, burns, or after mass excision due to the thin envelope of the skin. Surgeons have to perform reconstruction early to protect the underlying structures and preserve the functioning of the hand. There are many surgical techniques for dorsum reconstruction on the hand. The choice of the appropriate technique to address an injury depends mainly on the size of the defect. In mid-size defects, as in the case we report here, skin grafts, regional flaps, and free flaps are usually considered for reconstruction.
Split thickness skin grafts are required for patients with a granulation wound with a vascularized bed [1,2]. In our patient, who had exposed tendon and bone, reconstruction using a flap with good circulation was needed because a skin graft would have failed due to insufficient neovascularization. Microvascular free flaps require long operation times and microsurgical techniques. Most flap areas are too thick to apply on the dorsum of the hand. In addition, as in our case, vascular damage may accompany the defect making anastomosis problematic. Our patient had a traumatic history for both of his legs and this ruled out the use of free flaps such as the anterolateral thigh free flap. Consequently, we chose the reverse radial forearm free flap for reconstruction.
The reverse radial forearm flap has been proven to be a very reliable flap for hand reconstruction and does not require microvascular techniques. It can provide robust tissue and retain sensation in the reconstructed area. Venous congestion, which can lead to flap necrosis or failure, is usually reported in distally based flaps. The venous flow of the reverse radial forearm flaps moves in the opposite direction. Consequently, congestion can occur in the peripheral part of the flap due to this reverse flow and can cause flap necrosis. In order to prevent this and to improve outcomes, sufficient venous drainage is very important.
Many attempts have been made to address the disadvantages of the reverse radial forearm flap such as biological leeches (Hirudo medicinalis) or mechanical leech application, hyperbaric oxygen therapy or supercharging [3]. The method we implemented was venous supercharging. The effectiveness of venous supercharging has been reported by several authors using the transverse rectus abdominus myocutaneous flap, sural flap, propeller perforator flap, and the deep inferior epigastric perforator flee flap [4-6]. Elevation of a venous supercharging flap is relatively quick and safe and does not sacrifice main vessels. Adding venous anastomoses, which is a simple and short procedure, may improve venous drainage, avoid venous congestion, and can lead to flap survival.
In the reverse flow radial forearm flap, venous outflow is mainly achieved via two venae comitantes. The cephalic vein does not play an important role in venous drainage. Based on a simple technique, anastomosis with the cephalic vein and the dorsal superficial vein can reduce the incidence of venous congestion as well as flap necrosis. We propose prophylactic venous supercharging as a safe and reliable option in reconstruction of the dorsum of the hand.