원위 요골 골절에서 요측 지주 금속판의 유용성: 적응증과 치료결과
The Usefulness of Radial Column Plate in Distal Radius Fracture: Indications and Results
Article information

Trans Abstract
Purpose
The most common surgical treatment for distal radius fracture is internal fixation using volar locking plates, but it is sometimes difficult to maintain reduction with them. Therefore, this research reports the results of surgical treatment with additional radial column plates.
Methods
We analyzed 12-month follow-up results in 100 cases. The patients had the B or C types of distal radius fractures, in accordance with AO classification, and underwent surgical treatment at our hospital from May 2013 to December 2019. There were 16 cases of B-type and 84 cases of C-type fractures. Out of these, 87 were treated with volar locking plates (V group) and 13 had additional radial column plates (VR group). The results of surgical treatment were examined clinically by measuring the disabilities of the arm, shoulder and hand (DASH) and Mayo wrist score, and radiologically by measuring the radial length, radial inclination, and volar tilt, before and after surgery.
Results
After treatment, the radiographic average in the V group showed a radial length of 12.3 mm, radial inclination of 20.2°, and volar tilt of 5.8°, while the VR group showed 11.6 mm, 22.3°, and 9.0° respectively. A statistically significant difference was found in the DASH score, and the DASH score showed good results in the VR group.
Conclusion
Additional radial column plate fixation is worth considering because it provides clinically and radiologically satisfactory results in treatment of B and C types distal radius fracture involving articular surface.
INTRODUCTION
Distal radius fractures are the most common forearm fractures, occurring in both young adults and the elderly [1,2]. In the past, nonsurgical treatment has been regarded as a good option to achieve good results, but now it turns out that anatomical reduction is necessary to prevent posttraumatic arthritis, thus increasing the importance of rigid internal fixation [3]. In particular, recent research has found that volar locking plates decrease the occurrence of complications such as tendon irritation or disruption when compared to dorsal locking plates, and have become more preferable in distal radius fracture treatment [3,4].
However, treatment with volar locking plates alone is difficult to collect and fix the bones in their original position in intraarticular fractures or comminuted unstable fractures following high-energy injuries such as falls, traffic injuries, and sporting injuries. In particular, in the case of radial styloid fractures or fractures involving the articular surface, many studies [4,5] have been conducted with the development of devices, but there is no consistency in opinion on the types of plates and the surgical process.
Among the three-column theory of fractures of the distal radius, in which fractures are composed of three columns with each column needing reduction, has been presented [6-8]. Following this, the radial column plate was first suggested to stabilize the external column [9]. After that, many studies have begun to present the advantages of radial column plates [5,10]. Accordingly, this research aims to present the results of the treatment of distal radius fractures using both volar locking plates and radial column plates.
MATERIALS AND METHODS
This research analyzed 100 cases with follow-up results of patients who had distal radius fractures and underwent surgical treatment in Busan National University Hospital from May 2013 to December 2019. The present study is a retrospective case-control study conducted under the official approval of the Institutional Review Board (No. 2103-017-101) with the informed consent. Among these cases, 13 patients had internal fixation with volar locking plates and radial column plates, and 87 patients had internal fixation with volar locking plates alone. It is considered a good indication when the radial columna is unstable after fixing the volar plate. For example, when the screw of the volar plate fails to fix the radial styloid process, or when the screw of the volar plate is fixed with only one screw, but the reduction is unstable, it is considered a good indication. The decision to perform radial column plate fixation was mostly made during surgery. The average follow-up period was 25.5 months (range, 15–34 months). The average age of patients was 49.8 years (range, 23–59 years), with 58 male and 42 female patients. According to the causes of injury, there were 42 cases of falls, 25 cases of traffic accidents, and slip down in 33 cases. The fractures were classified as per the AO classification using plain radiographs in the anteroposterior and lateral planes and with computed tomography findings; 16 cases were B type and 84 cases were C type (Table 1).

Dermography of the study subjects
After surgery, the radiological findings were compared and analyzed by measuring the radial length, radial inclination, and volar tilt of the final follow-up, before and after surgery. The reason for the use of radial column plate fixation is to maintain reduction in radial styloid process fracture by using an additional plate. The difference was not considered postoperative rehabilitation because it was not fixed for early mobilization. Clinical examinations were performed by measuring the range of movement of intercarpal articulation (flexion-extension, pronation-supination, and radial deviation-ulnar deviation) during the final follow-up period. Functional examination was performed by measuring the disabilities of the arm, shoulder and hand (DASH) score [9] and Mayo wrist scoring system [10] during the final follow-up. The radiographic and clinical results were measured independently for each patient, and the mean and standard deviation of the values were calculated. In addition, Mann-Whitney U-test and Fisher exact test were used for statistical analysis. If the p-value was lower than 0.05, it was interpreted as statistically meaningful. IBM SPSS Statistics ver. 20.0 (IBM Corp., Armonk, NY, USA) program was used to analyze the statistics.
1. Methods of surgery
The surgery was performed using modified Henry’s approach. First, it approached the plane between flexor carpi radialis tendon and the radial artery. After manual reduction, the volar locking plate was fixed.
A dorsal approach to the radial column between the first and second extensor compartments was performed. While monitoring the branches of the superficial radial nerve, the fat and skin tissue were incised. The extensor retinaculum incision between the first and second compartments was minimal (Fig. 1).

Check the location and direction to avoid damaging the superficial radial nerve. Incise the extensor retinaculum in the shape of the figure above.
The first extensor compartment should be cautiously checked for injuries of the abductor pollicis longus and extensor pollicis brevis that may occur with unstable traction during surgery. While below-elbow traction and ulnar deviation were maintained, the radial height and tilt were checked, and the radial column plate was fixed directly below the first extensor compartment along the contour of the radial column. For volar locking plate and radial column plate, the products of Osteonic (Seoul, Korea) were used.
RESULTS
Right after the surgical treatment or after 2 weeks, radiographs measuring the average value of the volar locking plate group (V group) showed radial inclination of 20.2°, radial length of 12.3 mm, and volar tilt of 5.8°, while the volar locking plate and radial column plate group (VR group) showed 22.3°, 11.6 mm, and 9.0°, respectively (Table 2). In all cases, the intraarticular step off and gap that occurred after surgery were not observed during the follow-up period. No significant statistical difference was found in the radial inclination and radial length, but the volar tilt was significantly different from that of the VR group, which was much closer to the anatomical normal value (Fig. 2-Fig. 4). During the outpatient follow-up period, the last measured functional examinations of the DASH and Mayo wrist scores respectively showed an average of 18.8 and 78.5 in the V group and 8.3 and 91.1 in the VR group (Table 1). A statistically significant difference between the two groups was found, and the patients in the VR group showed much better functional recovery. No complications such as nonunion or deep infection at the surgical site were found. There was no case of plate removal due to irritation or pressure pain. Only two cases had paresthesia at the superficial radial nerve 1 to 2 months after the operation, but during the 6-month follow-up, the symptoms naturally reduced, requiring no additional operation.
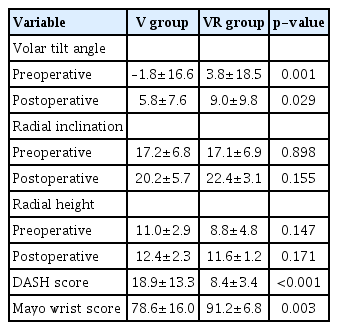
Radiologic and functional outcome

A 40-year-old man with unstable distal radius fracture was treated with open reduction and internal fixation using volar locking plate and radial column plate. (A) Preoperative radiographs show AO classification C3. (B) Immediate postoperative radiographs show successful reduction and fixation. (C) Radiographs at 13 months postoperatively show no significant loss of reduction. (D) Postoperative radiograph after metal removal operation.

A 53-year-old man with unstable distal radius fracture was treated with open reduction and internal fixation using volar locking plate and radial column plate. (A) Preoperative radiographs show AO classification C3. (B) Immediate postoperative radiographs show successful reduction and fixation.

A 59-year-old woman with unstable distal radius fracture was treated with open reduction and internal fixation using volar locking plate and radial column plate. (A) Preoperative radiographs show AO classification C3. (B) Immediate postoperative radiographs using external fixator. (C) Postoperative radiographs show successful reduction and fixation after external fixator removal. (D) Postoperative radiograph after metal removal.
DISCUSSION
Distal radius fractures in young adults are becoming increasingly complicated due to high-energy trauma such as industrial accidents, traffic accidents, and sporting injuries, which increase the incidence of intraarticular fractures or comminuted fractures. In older adults, the number of unstable fractures continues to increase due to the growing elderly population with increased life expectancy, in whom injuries are caused by simple falls because of osteoporosis [1,2,11].
Various surgical treatments of distal radius fractures have been developed. Percutaneous pin fixation has been a method of surgical treatment of distal radius fractures with the advantage of easy removal of pins after synostosis, which reduces the incidence rate of complications. Glickel et al. [12] showed that out of 55 patients, most achieved a superior result with only percutaneous pin fixation, while only four cases had displacement of fractures. However, Barton et al. [13] reported that percutaneous pin fixation is a minimally invasive procedure that reduces the incidence rate of complications. Nevertheless, for the treatment of severely comminuted fractures, it is difficult to maintain reduction, leading to malunion or dysfunction.
External fixation techniques were suggested by Anderson et al. [14] as a treatment for distal radius fractures, and the techniques have spread widely due to their simple surgical method and application in fractures with severe soft tissue injuries and open fractures. In addition, research has reported that these techniques combined with percutaneous pin fixation attain good results that are comparable to that of open reduction [15]. However, more research has started to report that displacement of fractures might occur after surgery in severely comminuted fractures [11,14,16], and with the development of more techniques such as open reduction and internal fixation using plates, its use is now less likely. Recently, surgical treatment with locking plates has been considered the best alternative treatment; it enables early wrist range of motion exercise and hand motion after anatomical reduction and rigid internal fixation [3,11,17].
The three-column theory explaining that distal radius fractures comprise of three columns was introduced by Rikli and Regazzoni [6,8] for treatment with a locking plate, and they emphasized that each column should be reduced for the treatment of distal radius fractures. However, it has been reported that distal radius fractures with radial styloid are difficult to apply plate fixation to after open reduction because the bone fragment is small and the plate screw could not get enough fixing force [10,16,18].
Helmerhorst and Kloen [9] reported that not enough research has been done for the treatment of fractures with radial styloid, but in their experience, using only volar locking plates makes it difficult to fix fractures with a small radial styloid. Grindel et al. [19] reported that using both volar locking plates and radial column plates showed structural stability improvement by more than 76% at extension, compared to treatment using only volar locking plates. Jacobi et al. [20] reported that a radial column plate should be used as a supporting plate for the treatment of comminuted fractures with radial styloid to help fracture reduction and maintenance because of good clinical outcome (visual analogue scale, Garland-Werley score, patient-rated wrist evaluation) and good radiologic evaluation (Dresdner Score).
This research showed the clinical results of the treatment of distal radius fractures with radial styloid using radial column plates, and the average values of the DASH and Mayo wrist scores were 8.36 and 91.15, respectively, which were satisfactory. If the radial styloid fragments are not fixed well, you can also simply Kirschner-wire (K-wire) pining. In this study, the buttressing was reinforced using a radial column plate because the comminution was severe and the fragment was small, so the fixation angle did not come out and the fixation force was weak when only K-wire pinning was performed. The screw of the volar plate could not be firmly fixed to the radial styloid fragment, but the addition of the radial column plate is thought to have played a role in reducing and maintaining the intraarticular displacement by collecting and supporting the comminuted bones. Due to the small number of cases, a limitation of this research, it was not possible to explain why the difference in clinical scores between the two groups.
Wei et al. [16] compared 12 cases of patients with unstable distal radius fractures who had volar locking plates and another 12 cases who had radial column plates. The short-term DASH score was higher in the group with volar locking plates but on the long-term follow-up period, both groups showed satisfactory clinical and radiological results. However, the research did not study the use of both volar locking plates and radial column plates together.
Galle et al. [18] reported that 27.8% of the patients who had surgical treatment with radial column plates had developed complications such as symptoms similar to those seen in De Quervain’s syndrome, paresthesia, and pain during activities. Therefore, they required an operation for removing the plate.
Helmerhorst and Kloen [9] reported that 14 patients who had operation with radial column plates did not show any symptoms similar to those of De Quervain’s syndrome or pressure pain at the plate fixed site, but two of them had a plate removal operation due to reduction loss and carpal tunnel syndrome. Fitoussi et al. [21] reported that surgery with dorsal plates showed 26% of rupture of the extensor and various other complications. However, research reporting that applying radial column plates would increase the rate of rupture of muscle is very rare [8,10,18].
When the screw of the volar plate fails to fix the radial styloid process, or when the screw of the volar plate is fixed with only one screw, but the reduction is unstable, radial column plate fixation is considered a good indication. The additional radial column plate is thought to have a good advantage as it acts as a buttress that reduces and maintains the displacement in the joint.
The limitation of this research is the small number of patients compared to the control group, which included 13 cases. Since it was a retrospective study, it was not possible to control the number of cases between each group, and there were no variables that could cause the difference between the two groups. Additionally, the bone mineral density of patients should be examined for the following comparative studies. In future research, more cases should be examined for the long-term follow-up period. In addition, we will consider how comminution degree, initial intraarticular displacement degree, high-energy injury, and ulnar side injury can have an effect.
CONCLUSION
In patients with unstable distal radius fractures with a radial styloid, if fixation with volar locking plates alone made it difficult to achieve anatomical reduction of the radial fracture at the distal radius, additional radial column plates fixation resulted in clinically and radiologically satisfying outcomes. Moreover, the results were statistically meaningful with less likelihood of reduction loss due to rigid fixation.
Notes
The authors have nothing to disclose.