INTRODUCTION
ANATOMY
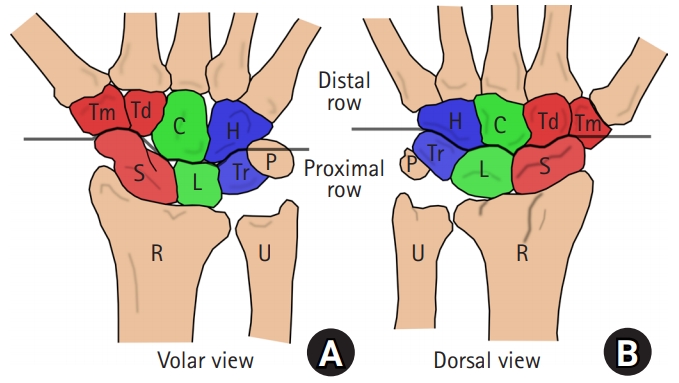
1. Carpal bones
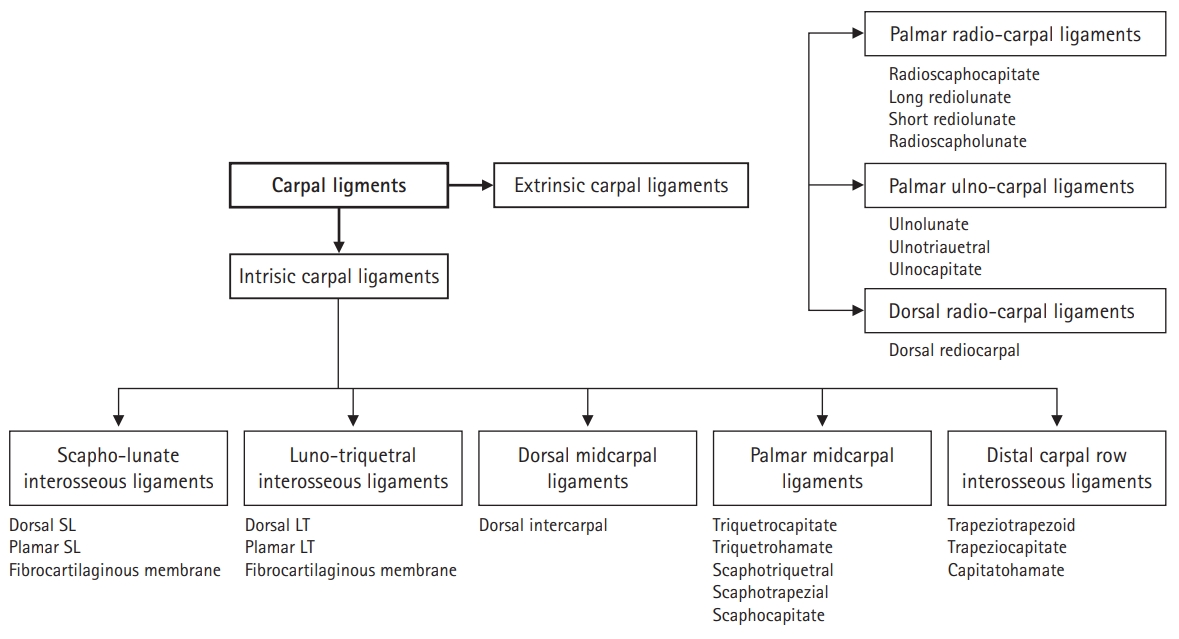
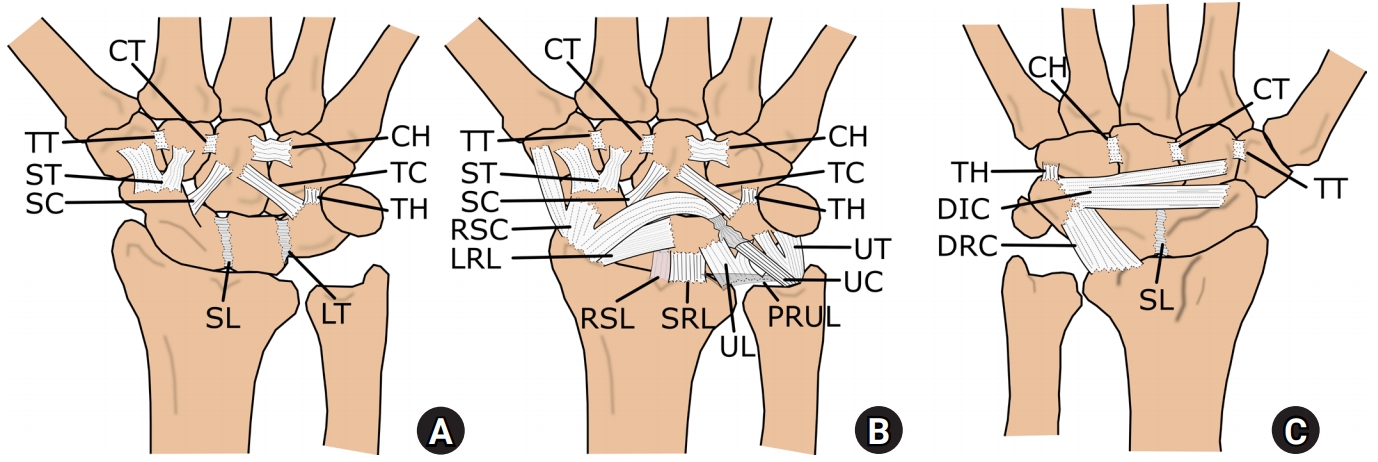
2. Carpal ligaments
Extrinsic carpal ligaments
① Palmar radiocarpal ligaments
② Palmar ulnocarpal ligaments
③ Dorsal radiocarpal ligaments
Intrinsic ligaments of the carpal bone
① Proximal interosseous ligaments
② Dorsal midcarpal ligaments
③ Palmar midcarpal ligaments
④ Distal carpal row interosseous ligaments
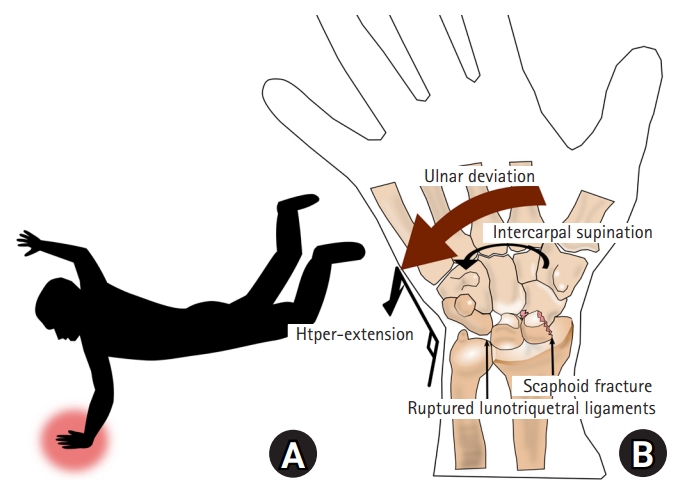
MECHANISM OF INJURY
CLINICAL PRESENTATION AND EVALUATION.
TREATMENT
SURGICAL TECHNIQUES
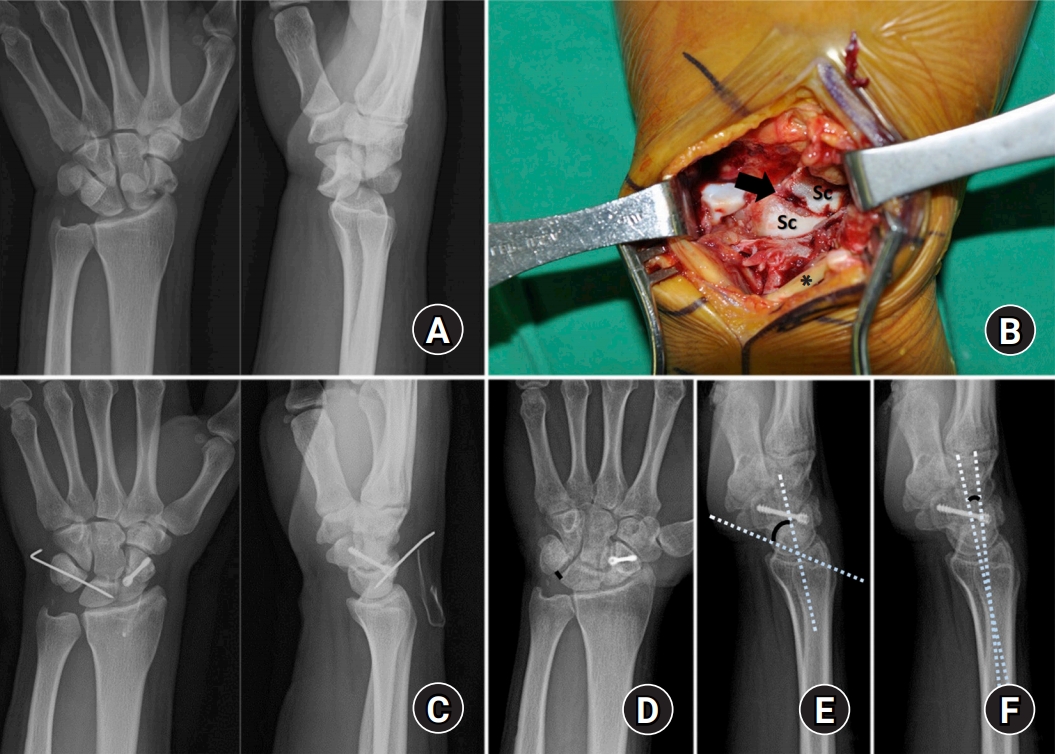
1. Anatomical reduction and fixation using dorsal approach (Fig. 7)
With the patient in the supine position, the arm was prepped and draped on a hand table. A pneumatic tourniquet and Esmarch bandage were used to exsanguinate the arm.
A 5-cm longitudinal incision was created on the dorsal aspect of the wrist in line with Lister’s tubercle. The incision was extended down to the extensor retinaculum.
The retinaculum was divided in line with the third dorsal compartment, and the extensor pollicis longus tendon was identified distally and retracted radially.
The second and fourth compartments were then reflected off the dorsal capsule. A capsulotomy was created and extended longitudinally.
Bone or cartilage fragments were removed from the joint, which was irrigated to remove any hematoma or other debris.
The scaphoid fracture was reduced using percutaneous joystick K-wires, and the guidewire for headless screw fixation was introduced along the long axis of the scaphoid.
After reaming, a headless compression screw (either an HCS 3.0 [Synthes, West Chester, PA, USA] or a Herbert mini screw [Zimmer, Warsaw, IN, USA] system) was inserted over the guidewire. The authors prefer cannulated headless screws over K-wires for scaphoid fracture fixations.
The LT joint was reduced and percutaneously pinned from the ulnar side of the wrist.
Capsulotomy incision was closed with interrupted absorbable 2-0 or 3-0 sutures.
The retinaculum was repaired, leaving the extensor pollicis longus free distally but still within its compartment proximally. The skin was then closed with nylon sutures.
2. Arthroscopic-assisted reduction and fixation (Fig. 8)
The patient’s arm was suspended in an Arc Wrist Tower (Acumed, Hillsboro, OR, USA) with 5 to 8 kg of traction after placing the index, middle, and ring fingers in finger traps.
A 3–4 portal, 6 radial (6R) portal, and midcarpal ulnar portal were sequentially created, and a 1.9-mm video arthroscope was introduced through each portal.
While using the midcarpal ulnar portal as the viewing portal, an STT portal or midcarpal radial portal (depending on the scaphoid fracture level) was created under direct vision as the working portal to facilitate the approach (Fig. 8B, 8C).
If present, bone or cartilage fragments and frayed edges of torn intrinsic or extrinsic ligaments that interrupted reduction were thoroughly debrided or removed to facilitate reduction of the scaphoid fracture or LT joint.
After releasing longitudinal traction, the scaphoid fracture was reduced with manipulation of the distal fragment using a probe, 18-gauge (G) needle, or percutaneous joystick K-wire under guidance from arthroscopic and fluoroscopic images.
A K-wire was subsequently inserted from the scaphoid tubercle and passed through the fracture site for temporary fixation (Fig. 8D).
After the arthroscopy switched into the STT or midcarpal radial portal, the LT joint was reduced using the same method and percutaneously pinned from the ulnar side of the wrist, starting at a point dorsal to the pisiform and aiming in a slight proximal direction (Fig 8E, 8F).
The arthroscope was introduced into the 6R portal to insert a guidewire for headless screw fixation of the scaphoid fracture.
The guidewire was percutaneously inserted through a 15-G needle, proximal and ulnar to the 3–4 portal, to target the ideal starting point at the most proximal tip of the scaphoid pole, immediately adjacent to the insertion of the SL interosseous ligament along the long axis of the scaphoid (Fig. 8G, 8H).
After removal of the provisional K-wire, a 5-mm transverse incision was made at the point of the prepositioned guidewire.
A sharp, straight hemostat was used to spread the soft tissue and pierce the dorsal capsule.
After reaming, a headless compression screw (either a Synthes HCS 3.0 or Acutrak mini screw system [Acumed]) was inserted over the guidewire to fix the scaphoid fracture.