INTRODUCTION
Autologous breast reconstruction with microsurgical flaps is commonly used after mastectomy in patients with breast cancer. This procedure is preferred because of better aesthetic outcomes which include softer, more ptotic, and natural-appearing breast mound [1]. Among the flaps, the deep inferior epigastric artery perforator flap has become increasingly popular over recent years.
As recipient sites for a free flap, internal mammary vessels and thoracodorsal vessels were utilized and internal mammary vessels were preferred due to low rates of vessel conversion and flap-related complications [2]. In the conventional method, the cranial limb of the internal mammary artery is used for anastomosis; however, successful arterial flow on anastomosis with the caudal limb of the internal mammary artery has been reported in several studies [3-5].
We present a case in which a salvaged deep inferior epigastric artery perforator free flap was used in breast reconstruction with retrograde anastomosis to the caudal limb of the internal mammary artery due to repeated arterial insufficiency on conventional anastomosis to the cranial limb of the internal mammary artery.
CASE REPORT
A 44-year-old woman was referred to our clinic for immediate breast reconstruction. She had invasive ductal carcinoma in the upper outer quadrant of her right breast and she was scheduled for total mastectomy. She had a history of cesarean section 7 years ago. We performed abdominal computed tomography scan for the evaluation of the internal mammary system and the deep inferior epigastric artery perforator and there were no abnormal findings in the arterial and venous systems (Fig. 1).
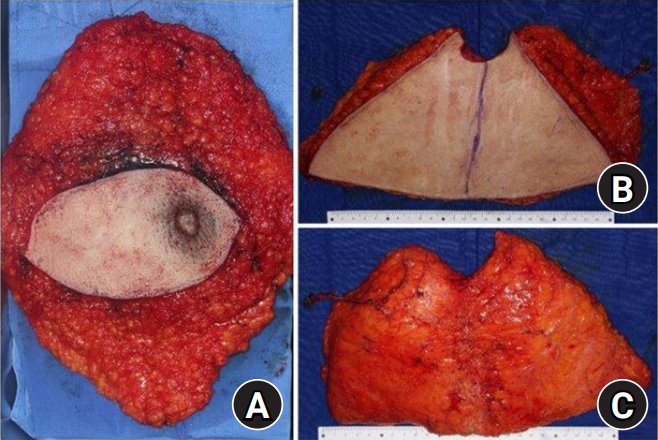
Total mastectomy was performed by the general surgeon and the mastectomy specimen weight was 505 g. The flap was elevated on two perforators of the deep inferior epigastric artery (Fig. 2). Recipient vessels, internal mammary artery and vein, were exposed by removal of a segment of the third costal cartilage. On arterial anastomosis to the cranial limb of the internal mammary artery with the end-to-end maneuver, arterial insufficiency occurred three times. After confirming that the cranial limb arterial pumping was good, anastomosis was performed, but the color of the flap was not good during flap insetting, so this process was repeated three times. We used the DeBakey vessel dilator to check vessel and the flow before the anastomosis was fine, but the flow after the anastomosis was consistently bad. The most likely cause is thought to be spasm, but further consideration is needed. We changed the recipient vessel to the caudal limb of the internal mammary artery and end-to-end anastomosis was performed. After arterial anastomosis, inflow into the flap was successfully established (Fig. 3). When anastomosis was performed in caudal limb rather than cranial limb, the flow was maintained well, so we think it was not a technical problem. Venous anastomosis was performed between deep inferior epigastric veins and internal mammary veins with conventional end-to-end anastomosis.
There were no postoperative complications such as hematoma, seroma, infection, thrombosis, or flap necrosis. She had a favorable long-term outcome at postoperative 6 months (Fig. 4).
The study was approved by the Institutional Review Board of Ajou Medical Center (No. AJIRB-MED-MDB-16-308) and performed in accordance with the principles of the Declaration of Helsinki. Written informed consent, including publication of the clinical images, was obtained from the patient.
DISCUSSION
After mastectomy, loss of the breast mound has psychosocial effects which are associated with anxiety and depression, and negative effects on body image and sexual activity [6]. After breast reconstruction, regardless of the timing and technique of reconstruction, patients showed high quality of life, better social adaptation and relationships, and sexual relationships [7]. According to the statistical report of American Society of Plastic Surgeons, the number of breast reconstruction surgeries in USA increased by 39% from 2000 to 2016 [8].
The breast reconstruction method should be selected after considering the patient’s preference, underlying diseases, patient’s age, location and type of cancer, the type of adjuvant therapy, and the size and shape of the native breast. These methods are largely divided into two types; implant-based reconstruction or autologous reconstruction. The deep inferior epigastric artery perforator free flap has been the first choice for autologous breast reconstruction. Koshima and Soeda [9] reported the first clinical application of the inferior epigastric artery perforator flap in 1989. It offers the advantage of preservation of the rectus abdominis muscle and results in less donor site morbidity such as herniation.
Use of the internal mammary system as the recipient vessel has become a common practice in autologous breast reconstruction. The internal mammary vessels are preferred over the thoracodorsal vessels because of their central location, reliability in terms of size and constancy, freedom in flap insetting, relative resistance to atherosclerosis, and preservation following radiation therapy and axillary surgery [10]. The conventional method uses the cranial end of the internal mammary artery for anastomosis. However, due to arterial insufficiency or need for an additional recipient in a bipedicled flap, the caudal end of the internal mammary artery was used as the recipient in several cases [3-5,9].
In our case, anterograde flow of the internal mammary artery was too weak to supply the flap in repeated reanastomosis with an unknown cause. We changed the recipient site to the caudal end of the internal mammary artery and the flow was successfully reestablished. In the long-term follow-up, the aesthetic outcome was satisfactory without any evidence of fat necrosis.
The internal mammary artery splits into two main arteries, the deep superior epigastric artery and the musculophrenic artery; and during their course, they show anastomosis with the intercostal arteries, giving off perforating branches in each intercostal space. These collaterals and two main arteries were considered responsible for the retrograde flow of the internal mammary artery [4].
In conclusion, retrograde flow of the internal mammary artery could be a reliable recipient site when an alternate recipient site is needed in case of insufficient antegrade flow of the internal mammary artery or an additional recipient site is needed in case of a bipedicled or stacked flap.