Introduction
힘줄의 연속성이 파괴된 경우 저하된 기능을 회복하기 위한 다양한 수술 방법들이 소개되어 있다. 그중에 힘줄의 결손이 커서 일차 봉합이 어려운 경우 힘줄 이전술 또는 힘줄 이식술을 통해 결손 힘줄의 재건을 도모하게 된다. 성공적인 힘줄 이전, 이식을 위해서는 인장강도(tensile strength), 두께(bulk), 중첩(overlap)이 중요한 요소들이다. 즉, 조기 관절운동을 통해 주위 조직과의 유착을 방지할 수 있을 정도로 충분한 강도를 획득하여야 하는데, 중첩은 많되 두께는 얇아야 마찰 및 유착이 줄어들어 힘줄의 활주 및 운동을 잘 수행할 것이다[1]. 이를 충족하기 위해 포장 주위 봉합법이나 측측 봉합법과 같은 힘줄을 봉합하는 다양한 방법들이 보고되어 왔고[2-5], Pulvertaft 봉합법 또한 1956년에 처음 소개된 이후로 힘줄 재건에 가장 많이 사용하는 방법 중 하나이다[6]. 측측 봉합법은 수행하기 쉽고 장력을 조절하기 쉬우나 최대 부하(maximum load)가 낮다는 단점이 있으며[7], 포장 주위 봉합법은 두께가 작고(less bulky) 장력은 강하다는 장점이 있지만 술기의 어려움과 공여 힘줄(donor tendon)의 굵기가 충분해야 수행할 수 있다는 것이 단점이다[5]. 기존의 Pulvertaft 봉합술은 공여부 힘줄이 같은 단면에서만 교차하여 처음 통과하는 봉합(weave)을 기준으로 추가적으로 형성되는 봉합들의 위치가 0° 또는 180°에만 위치하게 된다. 이때 단순히 봉합의 수를 늘리면 힘줄의 봉합 부위에서 한 방향으로의 크기와 마찰이 증가하게 되고 이는 유착을 형성하여 힘줄의 활주와 운동을 방해하게 되며[8], 또한 봉합이 통과한 방향에 수직인 방향의 장력에 대해서는 저항성을 강하게 갖지 못하게 된다[9]. 따라서 우리는 이와 같은 문제점들을 극복하고자 직교 통과 기법을 이용한 새로운 힘줄 봉합 방법을 소개하고자 한다.
METHODS
Ethics statement: This study was conducted after obtaining approval from the Institutional Review Board of Seoul National University Hospital (No. H-2207-124-1342). Written informed consent was obtained from the patient for the publication of this study including all clinical images.
1. Patients
2016년 1월부터 2021년 12월까지 힘줄 손상으로 인해 Pulvertaft 봉합을 이용하여 수술을 시행한 환자 22명을 대상으로 하였다. 남자 9명, 여자 13명이었으며 평균 나이는 60.6±14.8세(범위, 30–93세)였으며 6개월 이상의 추시 관찰을 한 환자들을 대상으로 하였다. 건 손상의 발생 원인으로는 원위부 요골 골절 10예(수술 후 발생 7예, 보존적 치료 후 발생 3예), 건의 직접 외상(열상, 둔상, 압궤상) 7예, 류마티스 관절염에 따른 원위 요척관절염 3예, 종양 1예, 신경 손상 1예가 있었다. 힘줄 이전술은 9예, 힘줄 이식술은 13예였으며 굴곡건 재건은 4예, 신전건 재건은 18예였다(Table 1).
2. Clinical measurements
수술 후 3개월째에 DASH (Disabilities of Arm, Shoulder and Hand) 설문지의 축약본인 QuickDASH를 측정하였으며 힘줄 이식술을 시행한 환자들과 힘줄 이전술을 시행한 환자들의 QuickDASH 점수에 대해서는 Mann-Whitney test를 이용하여 비교하였다. 또한 최종 추시 관찰 때까지 건의 재파열 여부, 감염, 건 관련 합병증(사두마차 효과, 봉합 부위의 증가된 부피로 인한 운동 제한 등), 구축 여부 등을 측정하였다.
3. Operative methods
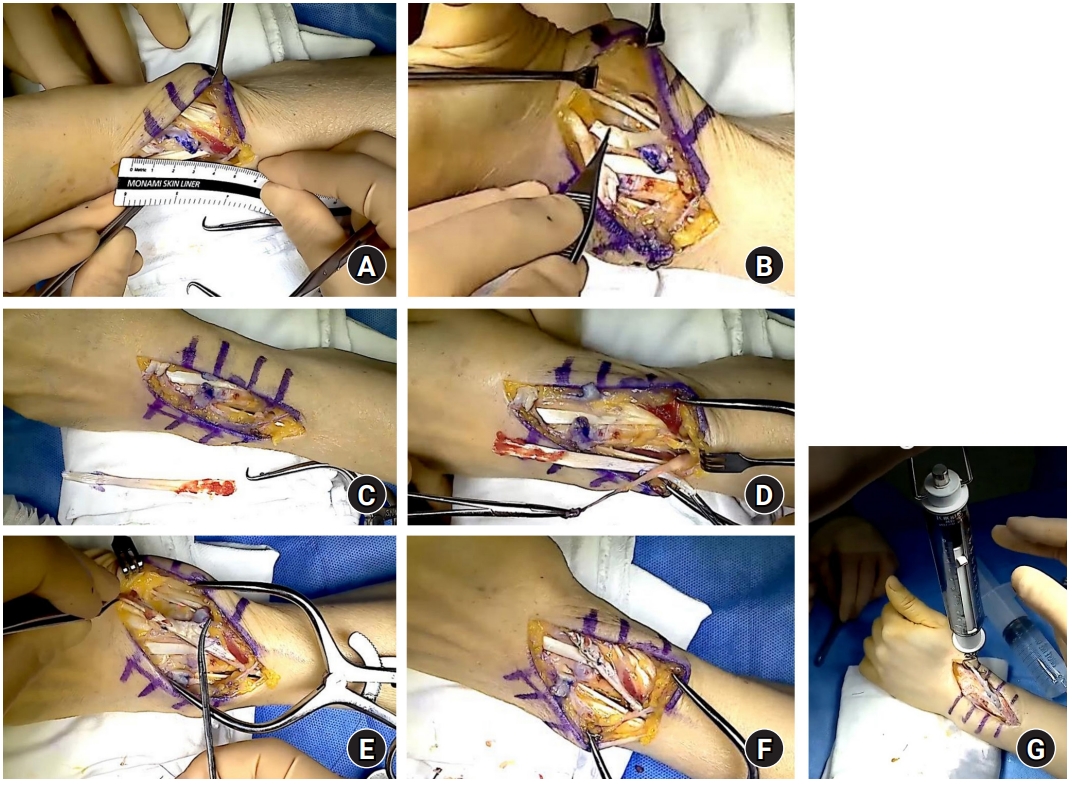
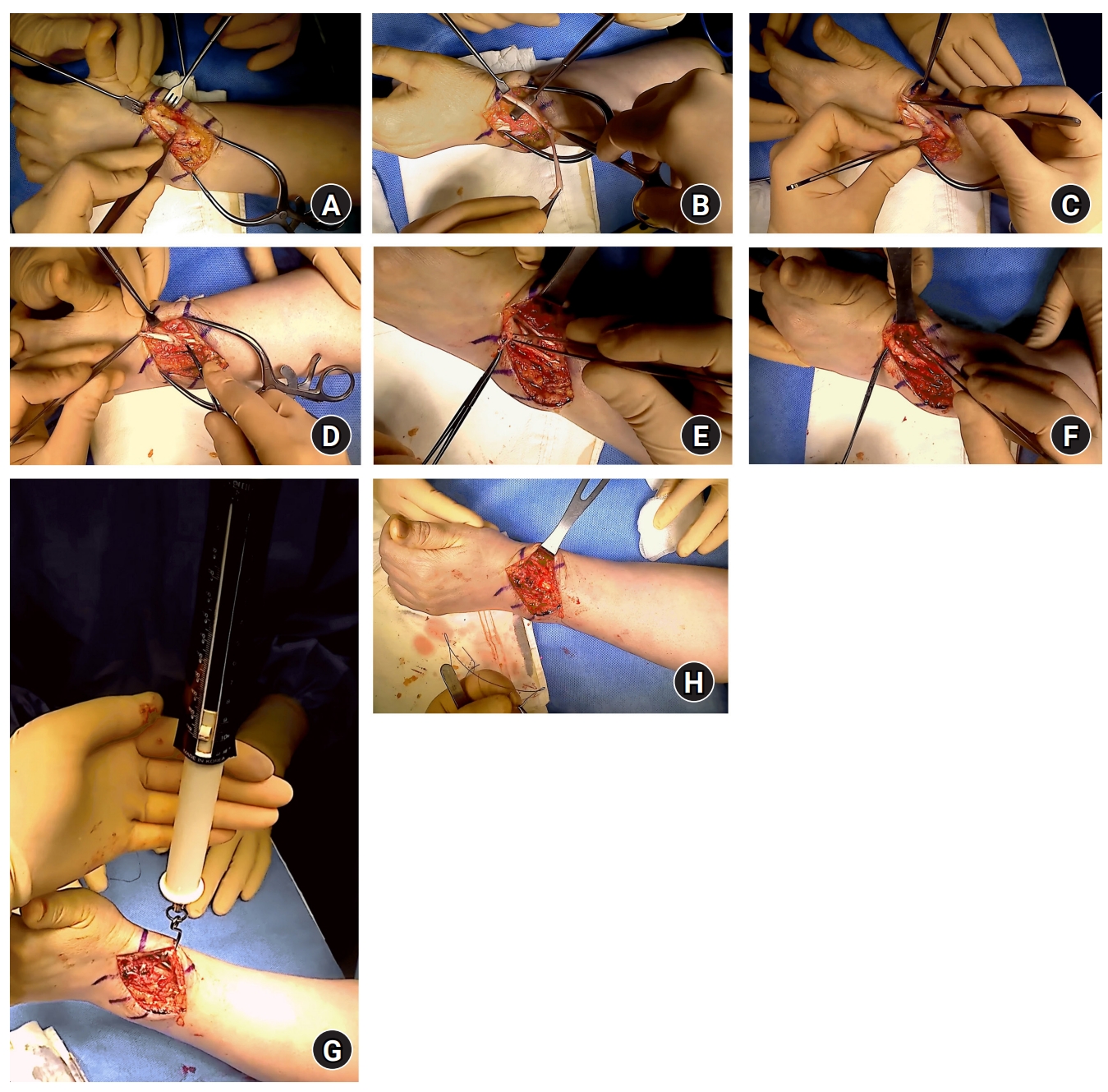
수용부 힘줄에 공여부 힘줄이 통과할 수 있는 힘줄 섬유의 방향과 평행하게 절개를 가한다. 수여부 힘줄에 절개를 가하는 위치는 기존 방법과 동일하게 시행하나 공여부 힘줄이 충분히 직교하면서 봉합되기 위해서는 기존에 사용하던 방법보다 더 긴 공여부의 길이를 확보한 상태에서 절개를 가해야 한다. 첫 번째 봉합은 바닥면과 평행한 방향으로 통과시킨 뒤 두 번째 봉합은 바닥면과 수직하게 통과시켜 두 번째 봉합의 교차된 봉합사가 힘줄의 바닥면에서 이루어지게 한다. 그리고 공여부 힘줄의 남은 길이에 따라서 같은 과정을 반복하여 공여부 힘줄이 수용부 힘줄을 두 방향에서 통과할 수 있도록 한다. 그리하여 추가적으로 형성된 봉합의 위치가 처음 형성된 봉합을 기준으로 각각 0°, 90°, 180°, 270°에 위치하도록 한다. 각각은 Prolene 3-0 또는 4-0 (Ethicon Inc., Somerville, NJ, USA)를 이용한 이중 매트리스 봉합 기법을 사용하였다. 이후 용수철 저울(Pesola Präzisionswaagen AG, Chaltenbodenstrasse, Swiss)을 이용하여 800 g 이상의 무게에 대해 저항성이 충분한지 확인 후 수술을 종료하였다(Figs. 1–3).
Results
1. Clinical measurements
수술 후 3개월째에 QuickDASH 점수를 측정하였다. 평균은 10.4±7.8점(범위, 3–22점)이었다. 굴곡건을 재건한 환자군(4예)은 평균 9.0±3.6점(범위, 4–12점)이었으며 신전건을 재건한 환자군(18예)은 평균 12.2±2.5점(범위, 4–28점)이었다. 또한 수상 원인이 외상인 환자군(17예)은 평균 11.1±5.8점(범위, 3–20점)이었으며 외상이 아닌 원인으로 수상항 환자군(5예)은 평균 13.4±5.4점(범위, 6–22점)이었다. 원위 요골 골절 환자군(10예)은 평균 10.6±3.7점이었고 원위 요골 골절이 아닌 환자군(12예)은 평균 12.5±6.9점이었다. 또한 힘줄 이전술 환자군(9예)은 11.3±4.4점, 힘줄 이식술 환자군(13예)은 11.9±5.9점이었으며 힘줄 이전술 환자와 힘줄 이식술 환자들의 QuickDASH 간에 통계적 차이점은 관찰되지 않았다(p=0.988) (Table 2).
재파열은 1예(case 16)에서 있었으며 장무지 신전건(extensor pollicis longus)이 리스터 결절(Lister’s tubercle) 주위에서 연장(elongation)되어 있었던 상태로 이에 대해 orthogonal Pulvertaft technique을 이용하여 봉합하였으나 다시 파열되었고 이에 대해 단 요 수근신건막(extensor carpi radialis brevis slip)을 이용하여 재건하였다(Fig. 4). 감염, 건 관련 합병증(사두마차 효과, 봉합 부위의 증가된 부피로 인한 운동 제한), 구축은 모든 증례에서 관찰되지 않았다.
Discussion
최근 들어 강도와 얇은 두께 둘 사이에 적절한 균형을 가지는 계단형 봉합법(step-cut suture)와 같은 얇은 봉합법들이 제시되고 있지만[10,11], 1956년에 Pulvertaft에 의해 소개된 이후로 강한 힘이 필요한 힘줄 수술에서 Pulvertaft 봉합법은 표준 치료로 되어 왔다[6]. 기존의 Pulvertaft 봉합법을 이용한 연구에서 힘줄 봉합의 강도와 부하에 대한 저항성은 통과하는 봉합의 수와 봉합사의 수에 비례한다고 보고하였고[12-14], 또한 건의 크기와 두께가 가장 중요하다고 하였다[15].
하지만 고전적인 Pulvertaft 봉합법은 하나의 단면만 공여부 힘줄이 통과하면서 연결되는 구조로 그 단면에 평행한 외력에 대해서는 저항력이 가장 강력하겠지만 봉합사의 매듭이 힘줄에 대해 분리되거나(slipping) 견인될 수가(pulling) 있다[16]. 그 단면에 수직한 외력이나 비틀림 부하(torsional stress)등에 대해서도 강력한지 의문이 생긴다. 또한 한 방향으로만 공여부 힘줄이 통과하게 되면 통과한 면에 대해서만 힘줄의 두께가 늘어나게 되어 활주의 제한과 유착을 초래하지 않는지도 의문이다[17-19]. 또한 이로 인해 봉합 부위 부피가 증가하여 힘줄 활주를 방해할 뿐만 아니라 힘줄의 혈류 공급에도 해로운 영향을 주어 힘줄 치유에 좋지 못한 영향을 미치게 된다[20-22].
이에 본 저자들은 Pulvertaft 봉합법을 변형하였다. 힘줄을 한 방향으로만 통과 방향을 한 방향으로만 하는 것이 아니라, 수직하는 두 개의 평면으로 힘줄이 통과하도록 하였다. 힘줄에 대해 견인력이 작용하였을 때, 힘줄이 견인되는 방향이 많아지게 되면 힘줄끼리의 저항이 더 커져서 견인에 대한 저항성이 클 것으로 생각하였다. 기존의 Pulvertaft 봉합법에 비해서 한 방향으로만 부피가 증가하는 것이 아니라 수직으로 통과하면서 부피가 두 면에서 모두 고르게 증가하여 한 면에서 활주의 제한이 일어나는 것을 방지할 수 있을 것이라 생각된다.
또한, 힘줄의 꼬이는 방향이 서로 직교하면, 두 힘줄 사이의 접촉면을 늘릴 것으로 생각된다. 이로 인해 늘어난 접촉면은 마찰력의 증가로 이어지면, 힘줄 사이의 유착 증대와 견인력 저항성 역시 증가할 것으로 기대하였다. 이는 향후 생역학적 실험과 측정 등의 증명 과정이 필요하다.
Savage [23]는 봉합된 건은 조기에 운동 프로토콜을 수행하기 위해서는 최소 75 N의 장력을 버텨야 한다고 보고하였다. 이에 본 저자들은 힘줄의 재건을 마친 뒤 용수철 저울을 이용하여 재건된 힘줄의 장력을 측정하였다. 최소 800 g 이상의 하중으로 지면과 수직된 방향으로 중력에 반하여 힘을 가하였으며, 중력가속도인 9.8 m/sec2를 곱하여 80 N 이상의 장력을 갖고 있는지를 확인하고 힘줄 재건을 완료하였다. 그로 인해 수술 직후부터 조기에 능동적 운동이 가능하여 좋은 기능적 회복을 가져올 수 있었다[24-26].
본 연구의 제한점은 다음과 같다. 첫 번째로는 후향적 연구로 처음부터 대조군을 통제하여 동일한 조건에서 같은 술식을 시행하여 비교하지 못하였다는 점이다. 두 번째로는 비교적 적은 크기를 대상으로 한 연구라는 점이다. 세 번째로는 직교 통과 기법을 이용한 수정된 Pulvertaft 봉합법에 대해 생역학적인 측정을 하지 못했다는 것으로, 이는 이번 초기 연구 이후 사체를 통한 생역학적 연구를 통해 1년 추시 때의 파악력(grip power)과 장력에 대한 저항성을 측정하여 종합적으로 분석할 예정이다. 네 번째로는 직교 통과를 할 정도로 공여부 힘줄이 충분히 긴 경우에만 사용할 수가 있다는 점이다. 공여부 힘줄 길이가 긴 경우에는 충분한 길이를 확보하여 수직으로 최소 4번 이상 통과를 할 수가 있으나, 힘줄의 퇴행으로 두께가 얇아지거나 유착 등으로 인해 공여부 힘줄의 상태가 우수하지 못할 경우에는 본 술식을 사용하는 데 제한이 있다. 그러나 본 연구에서 제안한 술식은 힘줄 간에 크기가 다른 경우에도 쉽게 사용할 수 있으며 힘줄의 두께가 얇은 경우에는 공여부와 수여부에 관계없이 얇은 힘줄이 굵은 힘줄을 통과하면서 직교 봉합하는 방법으로 문제를 해결하였다. 직교 통과 기법을 이용한 Pulvertaft 봉합법은 같은 단면에서 만의 교차를 통하여 봉합을 하는 기존의 Pulvertaft 봉합법에 비해 크기와 두께를 고르게 분산하여 한 방향에서의 마찰과 유착을 감소시킬 수 있으며, 수용부 힘줄에 대해 모든 사분면에서 이식 힘줄이 통과하여 힘줄이 통과하는 방향에 수직인 방향의 장력에 대해서도 구조적 안정성을 더 확보할 수 있을 것으로 보인다.