DEFINITION OF MICROSURGERY
Microsurgery encompasses all surgical procedures performed under a microscopic view in the fields of plastic and reconstructive surgery, otolaryngology, ophthalmology, neurosurgery, and urological surgery, among others. However, in a narrow spectrum, it refers to the surgical inosculation of microvascular, microneural, or lymphatic structures of less than 3 mm diameter under a magnified visual field [1]. The name microsurgery is often considered a synonym for reconstructive microsurgery.
Rapid progress has been made in the field of microsurgery as a result of diverse technological breakthroughs in surgical equipment. However, the history of microsurgery began even before the invention of the surgical microscope in the 1920s, as some surgeons used single-lens glasses and operating loupes for magnification in the 1870s [2]. The introduction of anticoagulants such as heparin in 1916 and the development of microsurgical instruments and suture materials in the 1960s accelerated the evolution [3].
Throughout the past half-century, microsurgery has accomplished astounding achievements in both quantitative and qualitative ways and has become an indispensable part of reconstructive surgery. However, microsurgery has its own drawbacks, including prolonged surgical time, specialized tool requirements, extended surgical training to achieve advanced technical skills, and suboptimal unsecured flap survival rates even in the best microsurgery centers, with 2% to 3% failure rates reported [3]. Despite these drawbacks, it has become a widely used form of surgical treatment in reconstructive surgery with continued advances in technology and higher success rates.
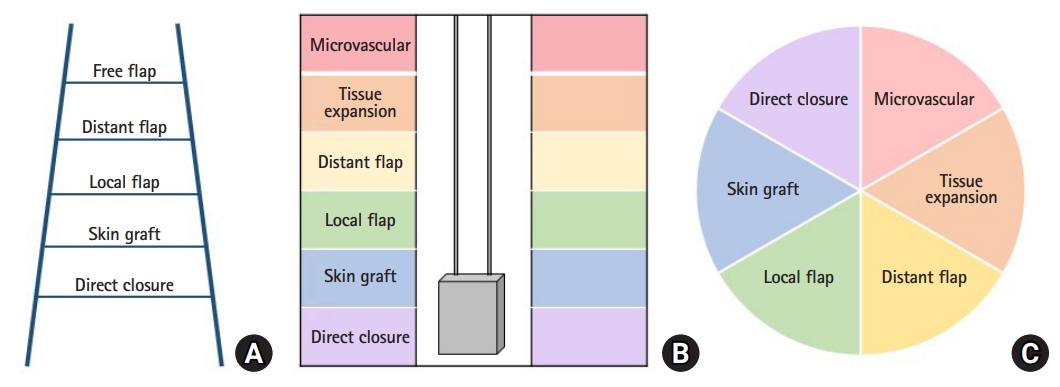
In the past, according to the concept of the reconstructive ladder, free flaps were considered as a secondary option for cases that required reconstructive surgeries where skin grafts or local flaps had failed to achieve acceptable results. The concept of the reconstructive elevator or reconstructive pie has been widely accepted, and reconstructive microsurgery is becoming one of the first preferences with excellent functional and esthetic outcomes (Fig. 1) [4].
In this article, the history and development of microsurgery, as well as recent advances and future directions, will be discussed.
DEVELOPMENT OF MICROSURGERY
1. Beginning period (the late 19th century to the early 20th century)
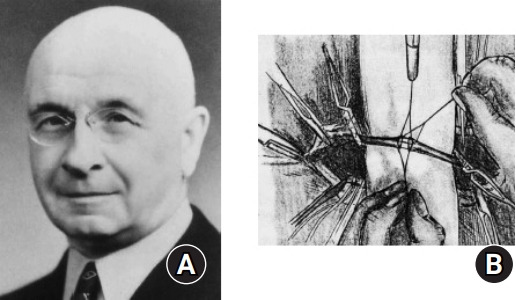
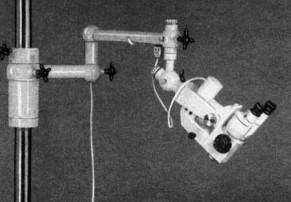
The origin of microsurgery can be traced back to a period between the late 19th century and the early 20th century when specialized surgical instruments, anticoagulants, and intraoperative magnifying devices were introduced (Table 1). Murphy [5] reported the first successful clinical case of end-to-end vascular anastomosis in 1897. Carrel [6] won the Nobel Prize in 1912 by introducing the triangulation method, in which three equidistant stay sutures were placed first and fine sutures ran along the relatively flat surface between each of the stay sutures (Fig. 2). This method laid the groundwork for organ transplantation and heart surgery. In 1916, McLean [7] fostered an essential step forward in the progress of microvascular surgery by discovering heparin. Subsequently, Holmgren [8] and Nylen [9] reported cases of successful otologic and ophthalmologic surgeries performed using a monocular microscope in the 1920s. The foundation of microsurgery was finally established with the invention of the first operating microscope by Carl Zeiss in 1953 (Fig. 3). In the 1960s, Malis [10] developed the bipolar electrocauterization device for use in microsurgical procedures.
2. Dawning period (the late 1950s to 1970)
In 1960, Jacobson and Suarez [11] reported the first successful case of microvascular anastomosis of the carotid artery in a dog under a microscope. In addition, Jacobson was credited as the first person to use the term “microsurgery.”
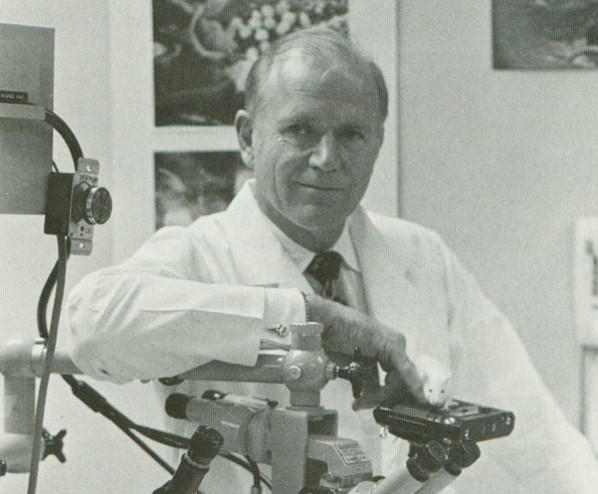
One of the first clinical applications of microsurgery involved replantation of amputated limbs, starting from vessels with relatively large diameters in the proximal part of the limbs to those with smaller diameters in the distal part. In 1962, Malt and McKhann [12] successfully performed the first arm replantation, involving microvascular anastomosis of the axillary artery and two veins of a completely amputated arm in a 12-year-old boy. Meanwhile, in China, Chen [13] managed to revascularize a completely amputated hand at the level of the distal forearm in 1963. Kleinert and Kasdan [14] successfully anastomosed an incompletely severed thumb in 1964, while in Japan, Komatsu and Tamai [15] successfully replanted a completely amputated thumb in 1965 (Fig. 4). In the 1960s, Buncke and Schulz [16] became the “founding father of microsurgery” for his establishment of the principles and techniques of replantation and transplantation through numerous animal experiments, as well as for his contribution to microsurgical training and education (Fig. 5). Hence, with such successes in microsurgical replantation, reconstructive microsurgery became a favorable treatment option worldwide.
The realm of microsurgery began to expand from replantation to free-flap transfer when Krizek et al. [17] reported an experimental case of free abdominal skin flap transplantation performed by anastomosing the superficial epigastric vessels to the carotid vessels in a dog in 1965. In 1966, Chen [18] successfully reconstructed a thumb using a second toe, and Cobbett [19] performed the first great-toe transfer in 1967. With these continued successes in replantation and free tissue transfer, the world’s first panel on microsurgery was held at the American Society of Plastic and Reconstructive Surgeons Annual Meeting in 1967, and the first International Microvascular Transplantation Workshop was organized in 1970.
3. Developing period (1971 to 1980)
Microsurgery made significant advances in the 1970s. In 1971, Strauch [24] worked on the first case of a vascularized bone transfer by reconstructing a mandible with a pedicled vascularized rib transfer in a dog. In 1972, Tamai [25] performed a free vascularized knee joint transplantation in a dog, demonstrating the possibility of a vascularized joint transfer as well as a vascularized bone graft.
With a better understanding of vascular anatomy, more innovative forms of free-flap transfer began to be introduced in various clinical situations. McLean and Buncke [26] reported cases of scalp reconstruction with greater omentum transfer, and Daniel and Taylor [27] reported the first successful free groin skin flap transplantation in 1973. A free pectoralis major muscle transfer was reported in China in 1973, followed by a gracilis muscle transfer for facial reanimation by Harii [28] in 1976. Harii’s gracilis muscle flap was the first functional flap to restore the function of the defect site by dynamic reconstruction in a patient with facial paralysis. This was a milestone that transformed the utility of free-flap transfer from mere coverage of soft tissue defects to the functional restoration of severed body parts.
In 1975, Taylor et al. [29] performed the first fibular free-flap transfer, and Baudet et al. [30] introduced the term “musculocutaneous flap” by describing a latissimus dorsi musculocutaneous flap in 1976. In 1977, Tamai [31] successfully replanted an amputated penis and scrotum. Shortly thereafter, both the iliac bone osteocutaneous flap (described by Taylor and Watson [32]), and the tensor fasciae lata musculocutaneous flap (described by Hill et al. [33]) were introduced.
In the late 1970s, replantation surgery became prevalent worldwide, and postoperative rehabilitation therapy began to be discussed. There were also further developments in peripheral nerve repair. Millesi [34] reported numerous experimental and clinical cases of nerve repair and nerve transfer.
In 1972, the International Society of Reconstructive Microsurgery was founded by orthopedic and plastic surgeons. The symposium continued to be organized biannually until 1999, when it merged with the International Microsurgery Society in 2001 to become the World Society of Reconstructive Microsurgery of today.
4. Fully-matured period (1981 to 1997)
By the late 1980s, microsurgery approached a fully-matured period, with continued research and modifications of the originally described techniques of free-flap transfer, especially in the field of hand surgery. Urbaniak et al. [35] provided practical guidelines for managing ring avulsion injuries by reporting successful cases of digital revascularization in 1981. In 1980, to overcome the disadvantages of great-toe transfer, Morrison et al. [36] suggested a new method of thumb reconstruction using an iliac bone graft wrapped with a soft tissue flap harvested from the great toe. Shortly after, Wei et al. [37] reported an alternative method of using the second toe-wrap-around flap, and Tsai et al. [38] succeeded in digit reconstruction by elevating the proximal interphalangeal joint of a toe in the form of a vascularized free flap in 1982. Through large-scale clinical studies, Godina [39] began to argue that early debridement and reconstruction with free tissue transfer, followed by aggressive rehabilitation, were the optimal treatment options for limb salvage. He also made a noteworthy contribution to reconstructive microsurgery as he reported the efficacy and safety of end-to-side anastomosis in free-flap transfers (Fig. 6) [40].
Continued contributions were made in an effort to minimize donor morbidity in free tissue transfers. In 1987, Taylor and Palmer [41] introduced the concept of a perforator map of the entire body, providing guidance for surgeons to safely design skin flaps based on angiosomes. This later led to the idea of a perforasome [42]. In 1983, Asko-Seljavaara [43] first introduced the term “free-style flap,” which was further advanced by Koshima and Soeda [44] who reported successful results using a deep inferior epigastric perforator flap in 1989, thus leading to the start of a new era of cutaneous perforator flap use. To minimize donor morbidity and produce a thinner flap, a venous-free flap, with no arterial structures and with arterial flow through only the veins, was introduced by a number of Japanese surgeons. Nakayama et al. [45] performed the first experimental venous free-flap transfer; Ji et al. [46] performed experimental flap transfers in rabbits; and Honda et al. [47] applied this technique in clinical situations in 1984.
THE EXPANSION AND RECENT ADVANCES OF MICROSURGERY
1. Supermicrosurgery
With a better understanding of angiosomes and the development of advanced microsurgical techniques, a new era of perforator flap surgery commenced. Supermicrosurgery began with the invention of surgical instruments for smaller vasculatures. In 1997, Koshima [48], in the first meeting of the International Course on Perforator Flap and Arterialized Skin Flaps in Belgium, reported that vessels with a diameter of less than 0.8 mm could be anastomosed safely (Fig. 7). Such procedures were later named supermicrosurgery, defined as techniques of microneurovascular anastomosis for vessels and single nerve fascicles sized 0.3 to 0.8 mm [49].
Supermicrosurgery offers the ability to manipulate small vessels that were previously inaccessible, making distal fingertip replantation possible [50]. Especially at the very distal tip of a digit where the vessel calibers are typically smaller than 0.5 mm, supermicrosurgical skills are essential to restore the form and function. Supermicrosurgery also enabled the elevation of smaller and thinner flaps possible, such as the super-thin superficial circumflex iliac artery perforator flap for reconstruction of subungual melanoma lesions [51]. It is now routinely used in a wide variety of microsurgeries, including lymphovenous anastomoses, vascularized lymph node transfers, and perforator-to-perforator anastomoses.
2. Lymphovenous anastomosis
Lymph node dissection has improved the overall survival of breast cancer and uterine cancer patients but has also contributed to lowering the quality of life of these patients by causing lymphedema. Lymphedema was considered an untreatable condition in the past; it was managed by nonsurgical physiotherapy, such as compressive wrapping or manual drainage, which only relieved discomfort temporarily. Although debulking of the edematous lesion and reconstruction with a skin graft (Charle’s operation) has been introduced as an option, its use is limited due to the nonphysiologic characteristics of the procedure and unaesthetic postoperative results. Liposuction can also be performed, but its effects are short lasting [52].
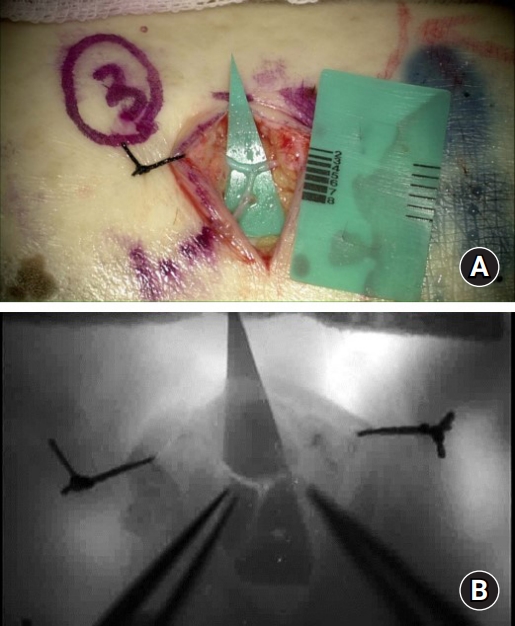
Lymphovenous anastomosis or lymph node transfer has been introduced as a result of progress in supermicrosurgery and the invention of evaluating tools such as lymphoscintigraphy and indocyanine green [53]. In 1990, O’Brien et al. [54] reported comparable results in the lymphovenous anastomosis of the upper and lower extremities. Today, it is one of the most popular treatment options for lymphedema (Fig. 8).
3. Composite tissue transplantation
With progress in immunology, composite tissue allotransplantation has become prevalent worldwide. The first hand transplantation was performed in 1998 by Dubernard et al. [55] in France (Fig. 9), followed by the second transplantation by Jones et al. [56] in the United States in 1999. The postoperative results were satisfactory in both esthetic and functional ways, and the conventional method of immunotherapy for acute rejection control was effective. Although there has been no mortality related to hand transplantation, two patients have undergone re-amputation due to immunosuppression-related complications.
More complicated and diverse forms of facial allotransplantation have been extensively studied and developed in Europe and the United States. Devauchelle et al. [57] succeeded in transplanting free soft tissue from a deceased donor to a woman’s lower face in France in 2005. The International Registry on Hand and Composite Tissue Transplantation reported 66 cases of upper extremity and 30 cases of face allotransplantations in 2017 [58]. In addition to soft tissues, various structures—including bones, cartilages, glands, and even the entire face—were transplanted to anatomical and functional deficit sites.
In South Korea, despite ethical and legal challenges, the first case of hand transplantation was performed in 2017 [59], followed by a second successful case in 2021 by the Severance Hospital team. However, controversy still exists regarding the practice of such transplantations for non-life-threatening reasons, considering the risk of side effects of lifelong immunosuppressive therapy. With technological breakthroughs in minimizing the complications of immunosuppressive agents, and developing immune-tolerance-inducing stem cell therapy, composite tissue transplantation will open a new field of microsurgery in the near future.
4. Robotic surgery
The application of medical electronic devices in the field of microsurgery has continued. Surgical robotic systems, such as the da Vinci Surgical System (Intuitive Surgical Inc., Sunnyvale, CA, USA), Zeus Robotic Surgical System (Computer Motion Inc., Goleta, CA, USA), and Automated Endoscopic System for Optical Positioning (Intuitive Surgical Inc.), which are in use today, were originally designed for remote surgeries during special situations such as wars. Theoretically, robot-assisted microsurgery has many advantages, including the availability of three-dimensional visual acuity with higher resolution, accessibility to challenging locations with minimal invasiveness, such as the deep and narrow intraoral spaces, and the ability to correct ineluctable minor intention tremor. However, robot-assisted microsurgery still has limitations even though almost 20 years have passed since its introduction. This is due to the lack of tactile feedback which enables the adjustment of tensions, the deficiency of appropriate surgical instruments, space-occupying problems of robotic devices, and high costs. In conclusion, although the advantages of robotic systems over the conventional method of manual suture are disputable, robotic surgery could revolutionize the field of microsurgery once some of its limitations are overcome [60,61].
5. Development of surgical devices
Although the application of microsurgery has become widespread, entry barriers are still high for beginners, with extensive training required. An increased duration of vessel anastomosis leads to an increased ischemic time, thereby leading to an increase in the total anesthetic time. A medical device called coupler GEM Microvascular Anastomotic COUPLER (Synovis Micro Companies Alliance, Birmingham, AL, USA) has been introduced to shorten the anastomosis time to avoid such occurrences. A systemic review on the use of couplers in vein anastomosis showed that the anastomosis time significantly decreased to an average of 5 minutes, with a thrombosis rate of 0% to 3%. The coupler also had a significantly lower rate of vein anastomosis failure than that of manual suturing (1.4% vs. 3.6%) [62].
MICROSURGERY IN KOREA
Professor Sun Lee (1920–2015), the renowned “Father of microsurgery in Korea,” graduated from the Seoul National University School of Medicine, then emigrated to the United States in the 1950s and became a pioneer in microsurgery. He is best known for his work in the field of experimental microsurgery with rat models and organ transplantation during the 1950s and 1960s. Microsurgery in Korea began as Lee visited Korea annually in the 1970s to train and mentor Korean surgeons in order to translate microsurgical techniques into clinical practice. The first Korean microvascular surgical workshop was held in 1975 (Fig. 10).
The first clinical case of replantation of an amputated thigh in Korea was performed by Yoo in 1976 (Fig. 11). The first toe-to-thumb transplantation was undertaken by Yoo et al. [63], and the first groin free flap for axillary scar contracture release was reported by Lim et al. [64] in 1978 (Fig. 11). The survival rate of the first cases of free-flap transfer in Korea in the 1980s was reported to be as low as 75%, which was not significantly lower than the rates reported worldwide at the time [65]. With more surgeons capable of performing microsurgeries and with further experience and skill acquisition in advanced techniques, the quality and quantity of microvascular transfers in Korea reached over the global-standard level in the 1990s and continues to progress even today [66].
The Korean Society for Microsurgery was founded in 1980 by 124 surgeons from the otorhinolaryngologic, urologic, obstetric, neurologic, orthopedic, and plastic surgery departments, all of whom practice surgeries using microscopes. Professor Man Kee Paik, an otologic surgeon, was the first chairman of the Society. Initially, the Society focused on almost any procedure performed under a microscope. However, as the symposium continued to be organized annually, discussions focused more on reconstructive microsurgery, and orthopedic and plastic surgeons took up the leading roles in the Society.
CONCLUSION
Since its beginning in the late 19th century, microsurgery has undergone significant development through a series of technological breakthroughs in engineering, surgical instrumentation, and medicine. Today, the application of microvascular surgical techniques in the fields of hand, plastic, and reconstructive surgery has resulted in revolutionary advances in allotransplantations and the replantation and transplantation of composite tissues. Not only has it become an indispensable part of modern surgery, but it also plays a pivotal role in the foundation of new surgical fields, such as lymphovenous anastomosis, and the development of new surgical devices, such as couplers. Microsurgery in Korea only began in the 1970s, but it has undergone rapid development and Korea has become one of the leading centers worldwide. Continued efforts to expand the application of microsurgery in clinical practice and research and to actively participate in the international arena will be the future of microsurgery in Korea.