Introduction
Schwannoma is the most common form of benign peripheral nerve sheath tumors. In rare cases, large, degenerative changes occur over a long period of time, resulting in a special histologic subtype termed ancient schwannoma. Ancient schwannoma was first described in 1951 by Ackerman and Taylor [1]. Since these masses are generally quite large at the time of presentation to a medical center, they can be easily mistaken for a malignant tumor on imaging tests or histological examination, requiring caution.
There have been two prior reported cases of ancient schwannoma arising from the distal ulnar nerve at the wrist level, but neither were long-standing or very large [2,3]. This may have been due to the fact that tumors that occur in the distal wrist are easily detected even when they are small. Therefore, there seems to be a lack of data on the clinical presentation and postoperative prognosis in patients with an ancient schwannoma of the distal ulnar nerve that has been left untreated for a long time and has grown very large. Herein, we present a case of a very large ulnar nerve schwannoma in a distal wrist and discuss the postoperative prognosis.
Case report
A 61-year-old man presented with complaints of tingling sensation of the fourth and fifth fingers and bulging of the ulnar side of the wrist. He said that the mass in his wrist grew very slowly, starting about 10 years ago, and that he had started experiencing a tingling sensation in his fourth and fifth fingers about 3 years prior, which had become worse in the past year. On physical examination, a 5 cm-sized mass was observed on the ulnar side of the wrist, showing a slight Tinel sign with no pain or tenderness. There was no evidence of ulnar or median nerve palsy in the hand.
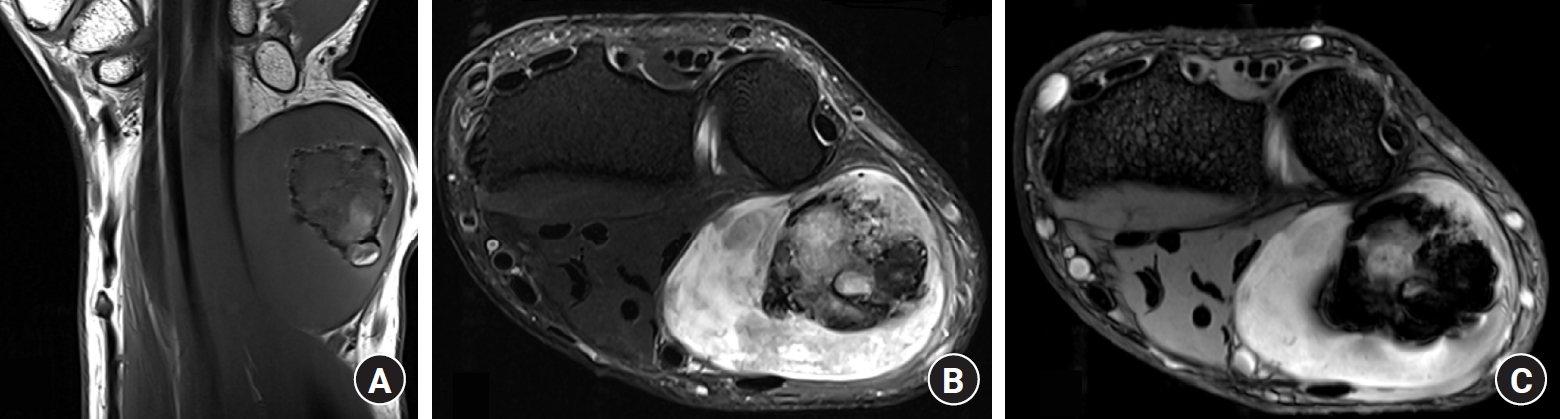
Several preoperative imaging tests were performed; the radiologic examination was unremarkable, while ultrasonography showed a 5.5×4.0×3.0 cm sized, well-defined mass containing internal hypoechoic areas. An ovoid heterogeneous mass measuring 5.5×4.5×3.0 cm was observed on magnetic resonance imaging (MRI). T1-weighted imaging (T1WI) showed an overall low signal intensity, T2-weighted imaging (T2WI) showed a mix of high and low signal intensity, and there were areas inside that showed low signal intensity on both T1WI and T2WI. Contrast-enhanced imaging revealed enhancement throughout the mass, except for some regions in the middle (Fig. 1). The tumor compressed the muscles and tendons, causing the ulnar side structures to deviate towards the radial side, but there was no invasion of the muscle or bone.
Based on the results of the preoperative examination, a benign nerve sheath tumor was suspected; however, due to the slight tingling sensation and the need to differentiate it from malignancy, it was decided to perform surgery. As it was thought that the possibility of malignancy was not high, we elected to perform a marginal excision and permanent biopsy with no frozen biopsy or wide excision. The surgical findings indicated a well-defined mass measuring 5×4×3 cm, which appeared to be eccentric with the nerves. Nerve fascicles were partially attached to the surface of the mass, and no fascicles were seen within the mass. The mass could be removed meticulously without causing any nerve injury (Fig. 2). Histologically, the encapsulated mass revealed nodular cellularity with streaming fascicles of spindle-shaped Schwann cells (Antoni A area) in the background of the myxomatous stroma (Antoni B area). Focally, a fibrinodegenerative paucicellular area and irregular vascular channels with hemosiderin-laden macrophages indicating a chronic process, consistent with ancient schwannoma, were observed (Fig. 3).
The patient still had a slight tingling sensation in the immediate postoperative period, but no other neurologic findings were noted. At his last visit 3 years after surgery, he reported no recurrence and that he felt better than before surgery, but some tingling sensations remained.
Written informed consent was obtained from the patient for the publication of this report including all clinical images.
Discussion
Ancient schwannoma is a variant of schwannoma characterized by slow progression and more frequent occurrence in the elderly. Schwannomas have no specific symptoms when small, but as they grow, they can cause symptoms such as Tinel sign, pain, and paralysis [4]. However, motor deficits, which occur mostly in malignant nerve tumors, are less likely to occur because the slow progression gives time for adaptation [5].
Ancient schwannoma has several characteristics which can aid in diagnosis. Antoni A area (dense hypercellular area with spindle cells) and Antoni B area (loose hypocellular area with myxoid tissue) appearing in an alternating pattern is a characteristic feature of conventional schwannoma [6]. Ancient schwannoma also shows an alternating pattern of Antoni A and B areas, but with relatively fewer Antoni A areas and a greater proportion of Antoni B areas [6]. In addition, slow growth and slow degenerative changes (cystic formation, calcification, hemorrhage, and perivascular hyalinization) may appear inside the mass [7].
In terms of imaging characteristics, first, ultrasonography shows a well-defined mass containing internal highly reflective areas or hypoechoic areas. MRI findings reflect the histologic features of schwannoma. Antoni A areas show a lower signal intensity on T1- and T2-weighted images, while Antoni B areas show lower signal intensity on T1WI and high signal intensity on T2WI. Hemorrhage, cystic change, calcification, and degenerative areas are heterogeneous but well distinguished from their surroundings. On contrast-enhanced MRI, Antoni A and B areas show contrast enhancement, while hemorrhaged or degenerative areas do not. The circumference of the hemorrhage or degenerative lesion is clearly enhanced, and the capsule in this area is usually also enhanced [7].
Ancient schwannoma can be mistaken for malignant tumors (malignant peripheral nerve sheath tumor, plexiform neurofibroma, malignant fibrous histiocytoma, etc.) on preoperative examination; as such, it is important to make a differential diagnosis on preoperative examination [8]. The key to preoperative differential diagnosis is performing imaging studies that reflect the patient’s age, time of presentation, presence or absence of neurologic symptoms, and the histologic features of the ancient schwannoma mentioned above.
At the time of surgical treatment, ancient schwannoma is often in an enlarged state; however, even enlarged tumors are not prone to complications such as motor deficits, which commonly occur in malignant tumors, because of ancient schwannoma’s slow progression [5]. Furthermore, even if the tumor itself is large, as was observed in this case, because most ancient schwannoma grow eccentrically, it is not difficult to excise without inflicting any nerve injury [2]. However, some minor injuries may occur after surgery, for the reasons mentioned: first, neuropraxia caused by intraoperative traction, second, injury to small fascicles when an incision is made in the capsule, and finally, the fascicle with the nerve sheath which the tumor originates should be removed with the tumor when it is removed [9].
Thus far, there have been two reported cases of ancient schwannoma of the ulnar nerve in the distal wrist [2,3], one of which was 1 cm in diameter and globular in shape, which the other was 2×3 cm and oval in shape, and both were less than 3 years old. The distal wrist is considered to be more susceptible to mass effects than the upper arm or proximal forearm as it has less free space and the surrounding tendons are not stretched. However, the two cases above were relatively small and quickly detected to cause mass effects or postoperative complications. Since the distal wrist had no free space and the mass was discovered and removed relatively quickly, it could not have grown large enough to cause degenerative changes for a long enough period of time as with an ancient schwannoma in a different region such as the proximal extremity. For this reason, cases of ancient schwannoma in the distal wrist that are sufficiently large and old to cause problems are rare and have not yet been reported. As opposed to the previous cases, the patient in this case report was neglected and underwent medical treatment relatively late despite the location in the distal wrist. As such, the mass was huge, raising concerns about potential problems caused by the mass effect before surgery or complications from the procedure during surgery. As there are currently no studies on ancient schwannoma in the neglected distal wrist, the clinical presentation, diagnosis and treatment process, and prognosis of this patient may be meaningful for the treatment of future patients.
The average life expectancy of people is increasing in many countries, including South Korea. In the past, ancient schwannomas, which occur predominantly in the elderly, were rare due to a lower life expectancy, but they may become more common and of greater clinical importance in the future. As such, an understanding of the clinical features of ancient schwannoma is important. As in the case of small ancient schwannoma in the distal wrist, most cases of large ancient schwannoma do not cause severe neurological symptoms and can be treated without special complications with a good preoperative diagnosis. However, if they are too old, as in the previously reported case in the upper arm that was over 40 years old, the nerves can become entangled in the tumor, resulting in postoperative complications [3]. Furthermore, in the distal wrist, a mass effect is likely to occur if it becomes too large. Therefore, if a mass suspected to be an ancient schwannoma is found in the distal wrist, even if it is large and old, it is expected to respond well to surgical treatment and prompt surgical removal is recommended.