Introduction
Releasing an ankylosed elbow is one of the most challenging procedures even for experienced surgeons. There are several etiologies for stiff elbow, such as trauma, infection, degenerative changes, heterotopic ossification, and congenital diseases [1,2]. The functional range of motion of the elbow joint is typically 30° to 130° [3] and surgical treatment is performed when there is no further improvement after a sufficient period of conservative treatment, or the patient cannot accept the result of the treatment. Anterior capsulectomy [4,5] and lateral [6-8], medial [9-11], posterior [12], and arthroscopic approaches [13-15] can be used to release ankylosed elbows. When determining the surgical approach, the nature of the stiffness, the location of the pathological structure, and any incisions from previous surgeries should be considered. Although capsulectomy by an anterior approach was introduced in 1948 [5], it has not received much attention recently. This is because the anterior capsule can also be accessed by a medial or lateral approach but when accessing the anterior capsule by methods other than an anterior approach, partial detachment of the common flexor or extensor muscular origin is inevitable [7,16,17]. We report the clinical results of a combined anterior and posterior approach, which allows safe access with good visibility, for severe elbow stiffness.
Methods
Ethics statement: This retrospective review was approved by the Institutional Review Board of Seoul National University Hospital (No. H-2011-105-1174). Written informed consent was obtained for publication of this study and accompanying images.
We retrospectively reviewed all patients who underwent surgical release by anterior and posterior approaches for elbow ankylosis at our hospital from August 2014 to May 2020. After a review of the electronic medical records and radiologic images, eight patients were enrolled in the study. Patients who had (1) articular incongruity of the ulnohumeral joint, (2) associated central nervous system injury, and (3) a follow-up period of less than 12 months were excluded. Five males and three females with mean age of 43 years (range, 21–65 years) were included in the study. Stiffness was associated with trauma in three cases, burn in one case, infection in one case, rheumatoid arthritis in one case, and birth palsy in one case. One patient presented with contracture that occurred after corrective osteotomy for a torsional deformity of the humerus 17 years prior (Table 1).
1. Preoperative assessment
The preoperative range of motion was measured using a large manual goniometer by one hand surgeon (JK). The average flexion contracture and further flexion were 53° (range, 30°–85°) and 95° (range, 35°–140°), respectively; and the average total arc of motion was 43° (range, 0°–80°). None of the patients had instability, neurological symptoms, or acute inflammatory signs at the preoperative physical examination.
In plain radiographs, we evaluated the congruity of the joint and assessed whether heterotopic ossification was visible on biplanar images. All patients had a congruent ulnohumeral and radiocapitellar joint surface except one whose radial head was impacted on the distal humerus due to sequelae of septic arthritis. Well-demarcated heterotopic ossification was identified in five patients. Two patients had heterotopic ossification in the olecranon fossa, posteromedial aspect of the capsule, and around the radial head; one patient in the olecranon fossa and posteromedial aspect of the capsule; one patient in the coronoid and olecranon fossa; and one patient in the olecranon fossa only. We did not routinely perform computed tomography (CT) before surgery, but in three patients, CT was conducted to determine whether the previous fracture was completely healed or to confirm the location of heterotopic ossification and congruity of the joint surface. In one patient with rheumatoid arthritis and another with a history of birth palsy, preoperative magnetic resonance imaging was performed to check for intraarticular pathologies or the condition of surrounding soft tissues. In the case of the sequelae of infection, blood tests confirmed that infection markers were in the normal ranges.
All of the patients were first recommended conservative treatment, and surgical treatment was indicated when there was no further improvement in the range of motion despite sufficient conservative treatment for at least 3 months. The Mayo Elbow Performance Score (MEPS), consisting of pain (45 points), motion (20 points), stability (10 points), and daily function (25 points), was used to evaluate total elbow function before surgery and at the time of the final follow-up. A score of 90 or higher was classified as excellent, 75 to 89 as good, 60 to 74 as fair, and less than 60 as poor [18]. The average preoperative MEPS was 43.8 points (range, 15–85 points).
2. Operative technique
A combined anterior and posterior approach was planned for patients with flexion and extension contracture, and an anterior approach was planned for one patient (patient 8) who had only 60°-flexion contracture without extension contracture. All operations were performed in the supine position under general anesthesia.
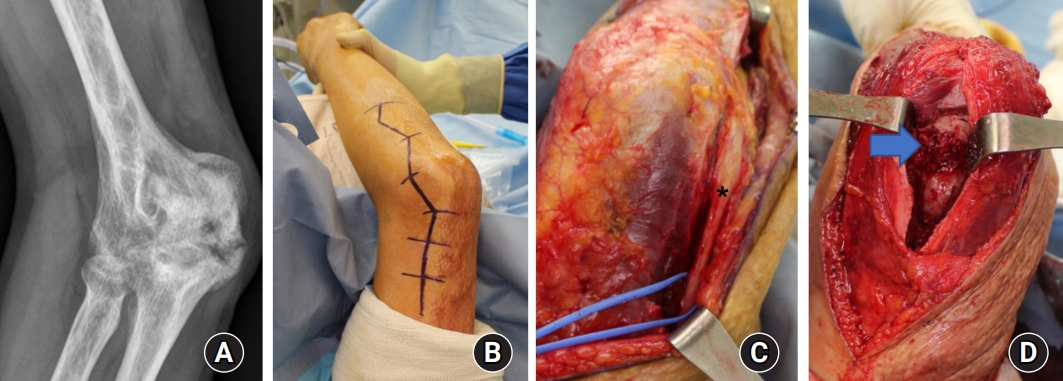
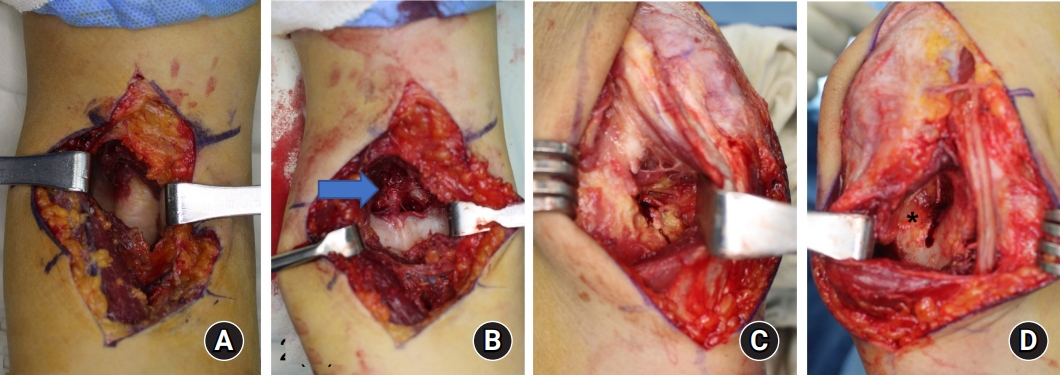
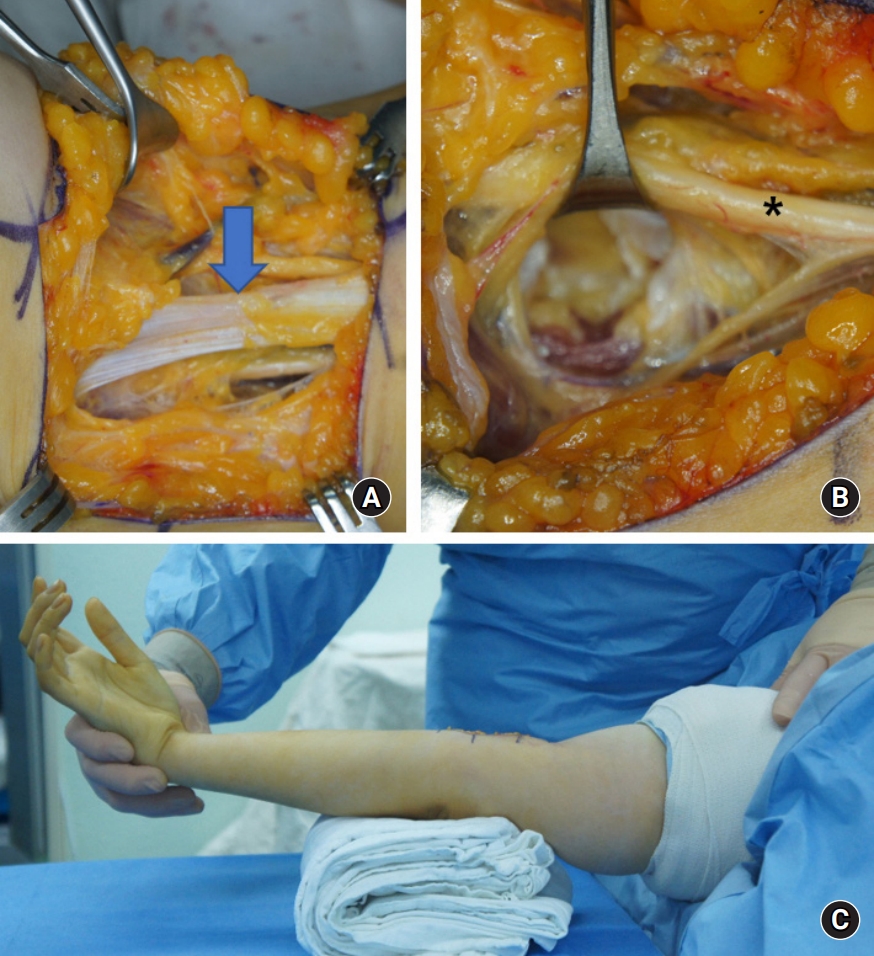
In the posterior approach, the incision line was made curvilinearly or in a zigzag fashion along the posterior midline of the elbow, avoiding the tip of the olecranon. The medial and lateral flaps were thickly lifted along the incision line, and the ulnar nerve was identified and protected. Although no patient complained of ulnar nerve symptoms preoperatively, the cubital tunnel was sufficiently released to avoid iatrogenic ulnar neuropathy caused by extensive contracture release. The heterotopic ossification of the posteromedial aspect of the capsule was removed along with the thickened posterior capsule, taking care not to damage the anterior band of the medial collateral ligament (Fig. 1). The triceps was elevated from the posterior surface of the humerus and heterotopic ossification with the fibrotic posterior capsule was removed to expose the olecranon fossa (Fig. 2). When impinging extension was still observed, olecranoplasty was additionally performed. An increase in the range of motion was confirmed at each step, and if necessary, the dissection was extended radially to excise the posterolateral joint capsule and heterotopic ossification around the radial head. In most cases, a sufficient range of motion was not achieved, even after releasing the posterior and posteromedial aspects of the capsule. The goal of the anterior approach was to sufficiently excise the thickened anterior joint capsule with heterotopic ossification of the coronoid fossa while protecting the neurovascular structures and minimizing damage to medial and lateral musculatures. A zigzag incision was made to avoid longitudinal scarring of the anterior elbow crease. The brachial artery running along the medial border of the biceps was identified and protected, and the brachialis was exposed by dissecting into the intervening interval. The brachialis was split or retracted laterally to fully expose the anterior capsule, and the thickened capsule was sufficiently excised (Fig. 2). In cases of severe adhesions, the median and radial nerves were identified and protected during the process (Fig. 3). After release of the contracture, the final range of motion was confirmed using the force of two fingers. We checked if there was subluxation of the ulnar nerve or excess tension on the ulnar nerve during maximum flexion after arthrolysis, and none of the patients underwent anterior translocation of the ulnar nerve.
3. Postoperative management
Postoperatively, a long arm splint was applied at a slightly extended from neutral position, considering the posterior incision. Active-assisted range of motion exercise was started 2 or 3 days postoperatively, and a night splint was applied depending on the contracture pattern of the patient. We did not routinely apply continuous passive motion to all patients but applied it for several days in patients who struggled with active exercise. All patients were advised to exercise on their own, and passive manipulation by the physical therapist was not performed in any case. A nonsteroidal anti-inflammatory drug was prescribed to patients who needed pain control during the exercise. Two patients received a 7-gray dose of radiation within 72 hours after the surgery as prophylaxis for heterotopic ossification.
Six months after the surgery, when the patient’s range of motion reached a plateau, the flexion and extension arc were measured by the same surgeon. The Wilcoxon signed-rank test was used to evaluate improvements in the range of motion and the functional outcomes after surgery.
Results
There was no significant difference in passive range of motion under anesthesia compared to preoperative measurement. In seven patients, contracture release was performed by a combined anterior and posterior approach, and in one patient who had only flexion contracture without extension contracture, only the anterior approach was used (Table 2). The location and pattern of heterotopic ossification in intraoperative findings were consistent with those confirmed by preoperative X-ray and CT.
There were three cases of stiff elbow related to trauma. One patient visited our hospital with severe stiffness that occurred after radial-head replacement due to a comminuted fracture (patient 3). X-ray showed a highly positioned radial-head prosthesis and heterotopic ossification in the olecranon fossa. The thickened capsule was excised and the prosthesis was removed with the adjacent fibrotic tissues. Another patient presented with complete ankylosis of the elbow after conservative treatment for a non-displaced fracture of the distal humerus (patient 1). By the anterior and posterior approach, heterotopic ossification of the olecranon fossa, posteromedial aspect of the capsule, and around the radial head were removed, and the range of motion was fully restored. The other patient had heterotopic ossification that occurred after surgical treatment for fractures of the distal humerus and the olecranon (patient 2). The preoperative range of motion was 50° of flexion contracture and 90° of further flexion. After surgical release by the anterior and posterior approach, the range of motion was restored to close to the normal range (Fig. 4).
A patient who had for more than 20 years suffered from sequelae of a septic elbow (patient 4) had complete ankylosis with the radial head impacted on the distal humerus. The radial head was excised by osteotomy of the lateral condyle, and internal fixation using a dual plate was performed. Six months postoperatively, a flexion contracture of less than 10° and a further flexion of 130° were obtained. In one patient with stiffness due to rheumatoid arthritis (patient 6), extensive synovitis was observed in the anteroposterior joint space and around the radial head. Open synovectomy by the combined anterior and posterior approach was performed (Fig. 2). Although this patient achieved a net improvement of 30° postoperatively, the arthritis was not controlled by medical treatment and stiffness recurred 2 years after the surgery.
In one patient with massive heterotopic ossification that occurred after a burn (patient 5), the range of motion was measured to be less than 5°. Because there was an extensive burn scar on the medial side of the elbow, the posterior incision was designed on the lateral side. The thickened anteroposterior capsule and heterotopic ossification were sufficiently resected, and a range of motion close to the normal range was obtained (Fig. 1).
One patient had stiffness caused by birth palsy (patient 8). The operative findings revealed severe contracture of the biceps muscle and fibrotic changes in the anterior capsule. By an anterior approach, resection of the thickened capsule and lengthening of the biceps tendon were performed, and the lacertus fibrosus was incised (Fig. 3). The other patient presented with stiffness, probably associated with a derotational osteotomy for congenital torsional deformity of the humerus 17 years prior (patient 7). Because contracture of the triceps muscle was observed in this patient, a posterior approach was made by triceps splitting, and aponeurotic lengthening was performed at the end of the procedure. Unfortunately, heterotopic ossification was observed on plain radiographs obtained 1 month postoperatively. Additional surgical release and postoperative radiotherapy were performed after maturation of the heterotopic ossification.
The mean follow-up period was 22.3 months (range, 12.1–36.9 months). In six patients, there was no further change from the range of motion measured 6 months after surgery, but in two patients the range of motion decreased at the last follow-up as a result of heterotopic ossification and the recurrence of rheumatoid arthritis, respectively. At the last follow-up, the average range of motion was 13° of flexion contracture (range, 0°–40°) and 123° of further flexion (range, 100°–140°). The average net improvement in total arc compared to preoperatively was 68° (range, –10°–130°). The mean MEPS was 89 points (range, 70–100 points), with the results rated as excellent in five, good in one, and fair in two patients at the time of the final follow-up, indicating significant improvement compared to the preoperative assessment (p=0.012). The two patients with fair results complained of mild pain, and their range of motion did not improve much due to heterotopic ossification and recalcitrant rheumatoid arthritis (Table 3).
Discussion
The anterior approach, which was introduced first, cannot theoretically solve the loss of flexion. Because the anterior capsule can also be accessed by the medial or lateral approach, the anterior approach is not commonly used alone, unless only flexion contracture is a problem or biceps lengthening is required [4,7,8,11,12]. The procedure for accessing the anterior capsule by medial and lateral approaches is basically the same, only the direction is different. During the procedure, the common muscular origin of the epicondylar area is partially divided, and the anterior capsule is carefully detached from the brachialis so as not to injure the neurovascular structures.
Although the incidence of heterotopic ossification according to approach has not been investigated, new-onset or recurrent heterotopic ossification is a poor prognostic factor for the outcome of surgical treatment for stiff elbow [17]. Abrams et al. [19] reported on risk factors for the development of heterotopic ossification after fracture fixation of the elbow. They found that a soft tissue insult, whether due to surgical dissection or the trauma itself, is often related to the development of heterotopic ossification, and that detaching or splitting the flexor-pronator musculature causes surgical trauma to the tissue, increasing the risk of ectopic bone formation. In this study, heterotopic ossification occurred in one patient who underwent aponeurotic lengthening due to triceps contracture (patient 7). Furthermore, there was a pronounced lack of cooperation in the rehabilitation process, and the final outcome was poor compared to the intraoperative findings.
Nerve complications are one of the most common complications of the open release of stiff elbow, and ulnar neuropathy accounts for the majority [20]. Known causes of ulnar nerve complication include iatrogenic injury during meticulous dissection and stretching due to postoperative improvement in the range of motion [21-23]. Aldridge et al. [1] reported that the median nerve was embedded in the anterior capsule due to severe scar formation in three out of 106 patients who underwent anterior surgical release for elbow contracture. Haapaniemi et al. [24] reported a case of complete transection of the median and radial nerves during arthroscopic release of posttraumatic elbow contracture. Although nerve injury after arthroscopic anterior capsular release is rare, attention should be paid not to injure the median nerve, posterior interosseous nerve, and brachial artery beyond the anterior capsule. Some of the patients included in this study had severe contractures of 60° or less, and three had complete ankylosis. In the anterior approach for these patients, we identified and preserved the neurovascular structures of the cubital fossa, and no neurological complications were reported in any of the patients.
This study was limited by the small number of patients and the heterogeneity of the study group. However, all surgeries were performed by one surgeon, and all patients were managed with the same postoperative rehabilitation protocol. Another limitation is that we performed radiotherapy in only two patients. We did not perform postoperative prophylactic radiotherapy at the early stage of the study, but we started doing so after experiencing a case of heterotopic ossification (patient 7). The other limitation is the short follow-up period. In the case of the most recently included patient, the follow-up period was 12.1 months, but the patient’s range of motion reached a plateau, showing good functional results. Considering these limitations, additional studies are needed to verify the safety and effectiveness of the combined anterior and posterior approach for releasing stiff elbow.
Conclusion
A thorough physical examination and surgical planning must precede the determination of a surgical approach for stiff elbow. When an extensive surgical release is required for severe contracture, a combined anterior and posterior approach may be helpful, allowing safe access with good visibility while minimizing the risk of neurovascular injury and preserving the medial and lateral muscles.