Introduction
Mycobacterial infection leads to a wide range of diseases in both immunocompetent and immunosuppressed individuals, with diverse symptoms. Skin and soft tissue infections (SSTIs) caused by mycobacteria include tuberculosis, nontuberculous mycobacterial (NTM) infections, and leprosy. These are caused by Mycobacterium tuberculosis (MTB), NTM, and Mycobacterium leprae, respectively [1,2]. SSTIs usually involve infection of the skin, underlying subcutaneous tissue, fascia, and muscle, but when exacerbated, bone or joint involvement may occur.
Mycobacterial infections are not rare, but SSTIs account for a low percentage of cases. SSTIs show nonspecific symptoms ranging from minor wounds, such as localized ulcers or abscesses, to systemic reactions in immunosuppressed patients [3-5]. In mycobacterial SSTIs, mycobacterial culture is the main method of diagnosis, but culture time can exceed several weeks and the detection rate is low. Due to this and the diverse clinical manifestations, timely diagnosis and treatment of mycobacterial SSTIs is challenging [1,4].
A combination of antibiotics has been suggested for mild forms of mycobacterial SSTIs [1-3,6-9]. Surgical intervention has also been recommended for abscesses, deep ulcers, or complicated cases such as those involving osteomyelitis or arthritis [1,4,6]. Unfortunately, a systematic approach has not yet been established for cases requiring such surgical intervention, making treatment in clinical practice more difficult.
Many studies have explored reconstruction of various compound and complex defects after infection. Good results have been obtained using microsurgical free tissue transfer as an advanced method [10-12]. For refractory mycobacterial SSTIs, however, treatment including such reconstruction has not been suggested; thus, in this study, we present a series of radical resections and reconstructions using a thoracodorsal artery perforator (TDAP) free flap as a resurfacing surgical strategy.
Methods
Ethics statement: The medical records and charts of patients were retrospectively reviewed after obtaining the approval of the Institutional Review Board of Hanyang University Medical Center (No. 2022-09-039). The study was performed in accordance with the ethical principles of the Declaration of Helsinki, and written informed consent for publication of the case reports with the clinical images was obtained from the patient.
1. Patients and preoperative assessment
Between December 2013 and February 2022, 13 patients presenting with mycobacterial SSTI underwent radical resection and reconstruction based on TDAP free flaps. Nine of these patients were male, and the mean age of the patients was 56.2 years (range, 31–77 years). All specimens submitted for identification of mycobacterial organisms were obtained in the form of tissue samples or discharge samples. For all specimens, acid-fast bacillus (AFB) stain and mycobacterial culture were performed. If positive results were obtained from either sample, polymerase chain reaction (PCR) were performed next to identify and classify the type of mycobacteria, also with a drug sensitivity test for applying proper antibiotics. In addition, after samples were tested for drug sensitivity, all patients were also given antibiotics in consultation with the infectious disease department. The infected sites were mainly on the extremities. The demographics and medical history data of all patients, including sex, age, etiology, identified Mycobacterium species, antibiotics applied, flap information, complications, and follow-up data were obtained by retrospective chart review. Detailed information on each patient is given in Table 1.
For exact mapping of the extent of the lesion caused by mycobacterial SSTI, preoperative magnetic resonance imaging (MRI) was performed. Bone or joint involvement and the extent of osteomyelitis and arthritis were accurately identified through MRI.
2. Surgical techniques
In cases without bone or joint involvement, where only soft tissue was infected, single-stage reconstruction was performed with resurfacing using free flaps immediately after resection. If bone or joint involvement was confirmed on preoperative MRI, two-stage reconstruction was performed. The infected lesion was first radically excised to eliminate additional sources of infection, and then negative-pressure wound therapy (NPWT) was applied. Resection of infected bone or joint was performed in cooperation with the orthopedics department. After that, when the wound bed was stabilized through NPWT and sterilization was confirmed with a negative AFB stain, the wound was resurfaced using a free flap.
Which free flap to use was determined according to the size and shape of the defect after resection. A TDAP free flap can cover defects of various sizes, but, in some cases, a chimeric flap or a latissimus dorsi (LD) musculocutaneous flap was more appropriate. A chimeric flap including the serratus anterior (SA) muscular component or fascial component was used when a small dead space was expected when applying only a TDAP flap or when functional support was required. When a large dead space was expected or a large volume of tissue was required for resurfacing, an LD musculocutaneous flap was used.
The initial settings for TDAP, chimeric, or LD musculocutaneous flap harvest were the same. Under general anesthesia, patients were placed in the supine position with the arm abducted and elevated. The lateral border of the pectoralis major and the anterior border of the LD were marked, and a line was designed along the midportion of the borders. A parallel incision was made along the midsection between the anterior border of the LD and the pectoralis major. At this point, identification of the anterior border of the LD is essential for successful flap harvest. Once the anterior border of the LD had been identified, the LD was pulled toward the surgeon. There were several perforators along the anterior border of the LD, and reliable, pulsatile perforators were selected and placed on skin paddles. The branch of the thoracodorsal artery pedicle that entered the perforators via the skin paddles was dissected. The avascular plane between the LD and the SA was easily dissected. The subscapular arterial system, including the SA branch, the circumflex scapular vessel branches, and the thoracodorsal vessels, could be identified. To obtain an acceptable-length vascular pedicle, vascular branches other than the thoracodorsal artery pedicle were ligated, while saving the thoracodorsal nerve branches. An outline of the flap was made on the skin paddle that would sufficiently cover the remaining defect. The flap was then harvested in the caudocephalic direction and detached carefully.
When harvesting chimeric flaps containing SA muscular components or fascial components, additional desired SA components were designed, and the vascular branches leading to the SA were preserved and elevated together. When harvesting the LD musculocutaneous flap, the LD muscular component including several perforators in the skin paddle was harvested along with the designed skin paddle. At this time, perforators were checked for branching from the thoracodorsal vessel without skeletonizing the perforator. The donor site was primarily closed or partially covered with skin graft followed by negative suction drainage.
After the harvested flap was positioned appropriately over the defect, the direction was adjusted to prevent kinking of the pedicle, and microanastomosis was performed with the recipient vessel in an end-to-end fashion with 9-0 monofilament nylon. Prostaglandin E1 was administered intravenously for 2 weeks postoperative.
Although radical excision was performed for the infected wound, in preparation for the slight possibility that the infection may remain, the surgical instruments used for the infected wound were not used during flap harvest to prevent donor site infection.
In the case of single-stage reconstruction, the patient was discharged after 2 to 3 weeks postoperatively. In the case of two-stage reconstruction, the period of NPWT application after radical excision was as short as a week or as long as 3 weeks, and after the reconstruction, the patient was discharged after observation for 2 to 3 weeks. After discharge, a close follow-up was performed at the outpatient clinic.
3. Antimycobacterial medication
Mycobacterial culture took about 4 weeks for identification of Mycobacterium, while PCR results took several days. If a positive result was obtained by chance in AFB stain performed for screening, PCR was carried out immediately and the result could be confirmed quickly. As soon as the results were confirmed, antimycobacterial medication was started in consultation with the infectious disease department. Additionally, as patients with mycobacterial SSTI may be accompanied by tuberculosis in other sites such as pulmonary tuberculosis, plain chest radiography was taken to check pulmonary or miliary tuberculosis in all patients with confirmed mycobacterial infection. Concomitant treatment with pulmonary or miliary tuberculosis was performed.
In the case of MTB infection, isoniazid, ethambutol, rifampicin, and pyrazinamide (abbreviated as HERZ) was used for 6 months because the treatment was the same as for pulmonary tuberculosis [2,8]. In the case of NTM infection, there were relatively many drug changes due to insufficient treatment establishment through a comparative randomized clinical study, but it was maintained for at least 2 months after surgery [2,4]. Patient compliance was checked during hospitalization and at the outpatient clinic of the infectious disease department. If other symptoms were present, the duration of use of the drug was also prolonged.
Since all MTB treatments are oral medications, the prescription during hospitalization and after discharge is the same, but in the case of NTM, there are medications that require intravenous injection, such as amikacin. If it was unavoidable, he visited the hospital every day, and injection was performed.
Results
1. Demographics
All patients with mycobacterial SSTIs were successfully treated with radical resection and resurfacing with free flaps. Causative organisms of mycobacterial SSTIs included species of MTB (n=8) and NTM (n=5). NTM species were Mycobacterium abscessus (n=3), Mycobacterium fortuitum (n=1), and Mycobacterium massiliense (n=1). In one patient with MTB infection, the infection recurred after primary resection and reconstruction, so treatment with resection and reconstruction using a flap was performed again. All flaps survived except for two cases of partial flap margin necrosis, which resolved with conservative treatment. The most commonly used flap type was TDAP only (n=10), followed by chimeric flap (n=3) and musculocutaneous flap (n=1). Flap size ranged from 7×5 cm2 to 25×12 cm2 (mean, 97.2 cm2). The mean follow-up period was 21.7 months (range, 12–42 months).
All patients had good compliance with antimycobacterial medications, but minor complications such as gastrointestinal trouble and skin rash occurred. These complications were resolved by altering the medication in consultation with the infectious disease department.
2. Case reports
Case 10
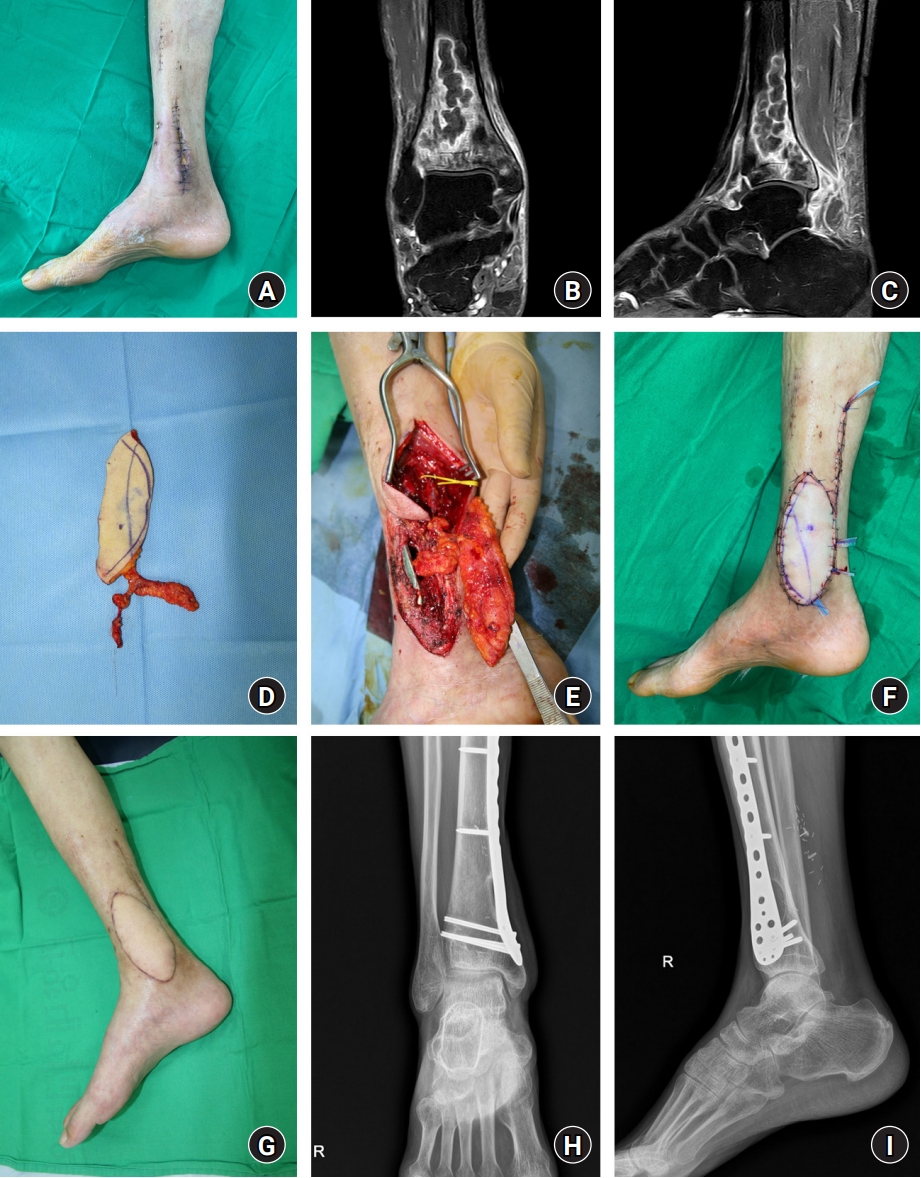
A 63-year-old man with a history of rheumatoid arthritis and diabetes was referred from the orthopedic surgery department. He had acute osteomyelitis of the right distal tibia, and was treated with vancomycin and gentamicin beads for 2 weeks, followed by internal fixation using a plate 1 month ago, but about 1×2 cm-sized wound dehiscence occurred repeatedly. Purulent pus-like discharge was observed in the wound, and MTB was identified on culture (Fig. 1A). Preoperative MRI confirmed remained osteomyelitis on the distal tibia (Fig. 1B, 1C); therefore, debridement and ostectomy was performed for radical resection, followed by NPWT application. After the wound was stabilized, a TDAP chimeric flap containing an SA fascial component was performed to resurface the defect, while SA fascial component covered the previously fixed plate (Fig. 1D, 1E). The posterior tibial vessels were used as recipient vessels. Two-stage reconstruction was successfully completed without any complications (Fig. 1F). Any recurrence or remained osteomyelitis was not observed at 1-year postoperative follow-up, confirming that resurfacing using a free flap to cover the defect was successful (Fig. 1G, 1I). Through a series of surgical interventions, the white blood cell (WBC) count and the C-reactive protein (CRP) level, which are inflammatory markers, were decreased from 8,700/mm3 to 5,100/mm3 and 7.1 mg/dL to 0.4 mg/dL, respectively.
Case 12
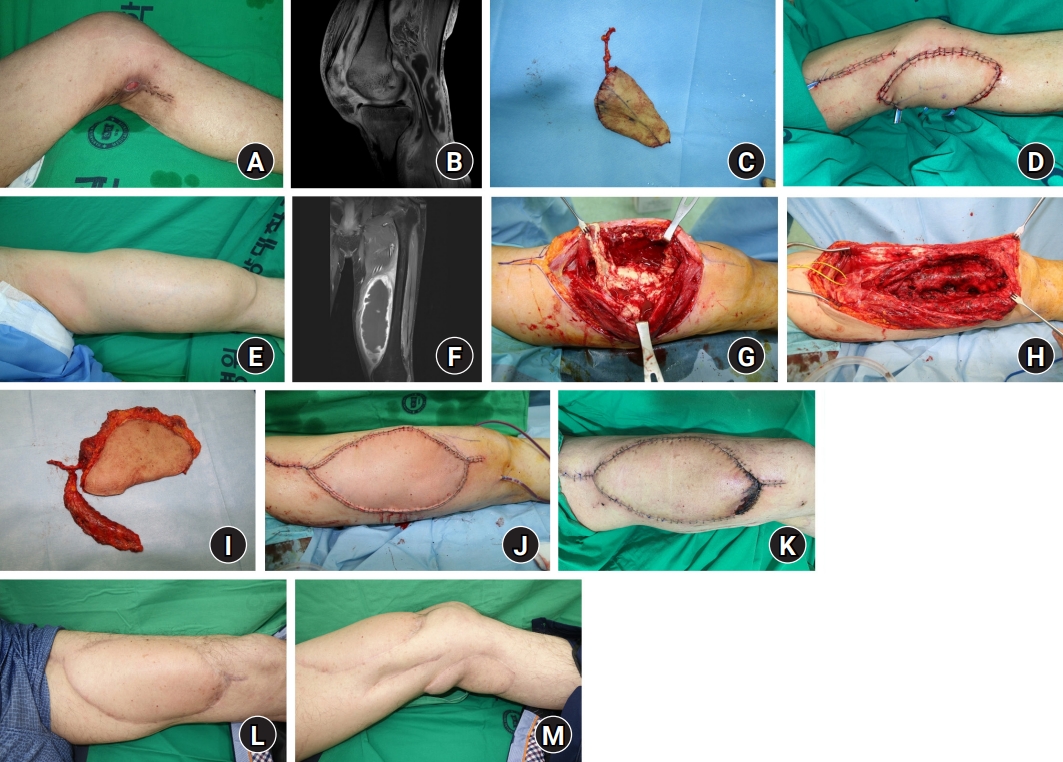
A 62-year-old man with a history of hypertension, diabetes, kidney transplantation due to end-stage renal disease, and miliary tuberculosis presented with 2×2 cm-sized left popliteal wound resulting from a scratch of unknown origin (Fig. 2A). As preoperative MRI and wound culture showed tuberculous arthritis of the knee joint, radical resection including bursectomy and NPWT was performed (Fig. 2B). A TDAP free flap was later used to cover the wound, with anastomosis to the medial superior genicular artery and greater saphenous vein (Fig. 2C, 2D). Through these surgical interventions, the WBC count decreased from 14,400/mm3 to 7,800/mm3 and CRP level decreased from 14.2 mg/dL to 0.5 mg/dL, which were normalized. There were no short-term complications, but swelling occurred in the medial thigh 11 months later (Fig. 2E). Follow-up MRI showed abscess formation arising from the suprapatellar bursa, and MTB was reidentified on culture of aspirated material (Fig. 2F, 2G). Definitive radical resection was performed through reoperation, and wound clearance was confirmed through NPWT (Fig. 2H). To cover the defect in the medial thigh, a TDAP chimeric flap containing an SA muscular component was used (Fig. 2I, 2J). The flap showed partial necrosis of the margin but healed without reoperation through conservative treatment (Fig. 2K). Any recurrence was not observed until 15-month follow-up after the second reconstruction, confirming that resurfacing using a free flap to cover the defect was successful (Fig. 2L, 2M). Through these second surgical interventions, WBC count decreased from 18,300/mm3 to 6,200/mm3 and CRP level decreased from 27.6 mg/dL to 0.3 mg/dL, which were normalized again.
Discussion
Concerns about the treatment of mycobacterial SSTIs are growing. Although the overall number of MTB-infected patients is decreasing, 5.8 million people were newly diagnosed worldwide in 2020. Of these, the proportion of SSTIs is less than 4%, but such infections are still often encountered in a clinical setting [13]. More than 170 species of NTM have been discovered, and although not all species are pathogenic and contagious among humans, the number of reports related to surgical, cosmetic, and other procedures is increasing [7,9]. As the prevalence of mycobacterial SSTIs is increasing in developed countries, mainly those associated with NTM species [14], an optimal and systematic strategy for treatment that can effectively cover defects occurring after infection needs to be established for cases requiring surgical intervention.
Previously, the focus of treatment was on the simple removal of infection through resection or non-surgical treatment with antibiotics only [5]. If the wound is infected with bacteria resistant to empirical antibiotics or if the wound is complex involving structures other than soft tissue, effective treatment will be delayed. As a result, the wound healing and hospitalization period of patients can be prolonged, which increases overall cost [11]. Long-term hospitalization and antibiotic use increase the incidence of various complications such as gastrointestinal problems, antibiotic resistance, and leukopenia [15]. For this reason, it is essential to carry out an appropriate culture, followed by drug sensitivity testing when the bacteria is identified, and to apply optimal antibiotics through consultation with the infectious disease department [16,17].
Even with appropriate antibiotics, severe SSTIs such as cases with abscesses, osteomyelitis, and arthritis are often not treated well with antibiotics alone and even worsened in many cases, requiring surgical intervention [18,19]. In the past years, treatment through serial debridement and secondary healing was applied, but the recurrence rate was high, resulting in poor outcomes and a long treatment period [20]. A regional flap was introduced as an alternative, and a radial forearm fascial flap was first used as a salvage procedure for cutaneous tuberculosis in 1998 [21].
An important aspect of our surgical treatment strategy is to remove the infection source as much as possible through radical resection, and to supply new vascularity to the wound bed through a microsurgical transfer of well-vascularized tissue. Our approach entails preoperative MRI prior to en bloc resection, and the timing of reconstruction is to be determined through this. Involvement of the bone or joint adjacent to the wound can be confirmed through MRI. In this case, NPWT was applied for complete infection control to minimize the possibility of remaining infected wounds and to prepare clean wounds after debridement [22]. Several weeks later, microsurgical tissue transfer was performed to complete a two-stage reconstruction. If the bone and joint were not involved, single-stage reconstruction was performed immediately after en bloc resection, with microsurgical tissue transfer to minimize the treatment period. Meticulous debridement and copious irrigation were performed in every surgery.
Through microsurgical tissue transfer, wound healing could be promoted by increasing blood flow, oxygen concentration, mobilization of WBCs, and phagocytosis around the wound bed [23]. In addition, because of the average antibiotic concentration around the wound, the activity of leukocytes and blood flow increased, making microsurgical tissue transfer the reconstruction method of choice in large and refractory infected wounds to reduce the risk of recurrence [10]. Also, well-vascularized tissue has been commonly used to promote wound healing and overcome local infections in chronic, unhealed wounds [19]. These points suggest that sterilization can be achieved through flap coverage in mycobacterial infected wounds. In addition, there is a cosmetic advantage because of the possibility of resurfacing to prevent discoloration, scarring, and joint immobilization that may occur during secondary healing [24].
In recent years, there have been rapid developments related to free tissue transfer, and many methods have been introduced. We chose reconstruction using TDAP flaps, which have several advantages compared with other flaps [25]. When the thoracodorsal axis is used, which includes the SA muscle and the LD muscle, chimeric or musculocutaneous flaps can be selectively harvested considering the shape, location, and functional characteristics of the defect [25-27]. In addition, we also used the “free style” flap design concept for harvesting TDAP flaps, which was described by Wei and Mardini [28]. It places emphasis on finding the perforator first and designing the flap later, depending on the location of the perforator. If a reliable perforator is found in that way, the flap can be designed parallel to the axis of the descending branch of the thoracodorsal vessels, having more options for choosing the shape and dimension of flap. Therefore, various flaps can be harvested according to the required amount and size of the tissue, making resurfacing easy and successful. Especially in wounds with osteomyelitis or arthritis, reconstruction can be performed to minimize the dead space for complex defects that may occur after en bloc resection using a chimeric or musculocutaneous flap. Since the donor site is located on the side, there is also a relative cosmetic advantage.
In the case of mycobacterial SSTIs, recurrence within 1 year is relatively common due to causes such as environmental influences and flora [2]. Considering the possibility of recurrence, even if complete en bloc resection is performed, serial outpatient-based observation is required. Since recurrence can occur at a location distant from the operation site, it is necessary to carefully examine the whole body to make sure that no other wounds occur during the follow-up period.
This study has several limitations. In this study, 13 cases were included in the study. However, we did not establish a control group without surgical intervention or a control group using a flap other than TDAP, and a rather small number of cases were included to accurately determine the effectiveness of TDAP. It is thought that the effect can be accurately confirmed through additional research in the future.
Thus far, no systematic and optimal treatment approach has been proposed for refractory and complex mycobacterial SSTI wounds. After radical resection, while using antibiotics against identified mycobacteria, reconstruction based on the TDAP flap can be the useful, cost-effective, time-saving, and successful resurfacing procedure for defects. We believe that this technique will be helpful to find the optimal treatment approach through future large-scale studies.
Conclusion
A systematic treatment plan has not yet been proposed for mycobacterial SSTIs requiring surgical intervention. In our study, it was shown that resurfacing the defects from mycobacterial SSTIs based on TDAP flap can be effectively performed while controlling infection through radical resection and application of antibiotics.