Introduction
Microsurgical reconstruction for traumatic soft tissue defects of hand is one of the most challenging fields for surgeons [1]. Traumatic hand defects usually have a complex level of injuries involving partial or total loss of local vasculature, tendon, or bone exposures which often requires free flap coverage [2]. While various parameters such as the magnitude of trauma, infection, postoperative management, and surgical judgment influence clinical outcomes, perhaps the most critical factors for flap success may be the surgical technique and recipient vessel status [1]. In terms of these two factors, the pediatric population is a particularly challenging subgroup [1].
Nowadays, thanks to the development of microsurgical tools and surgical techniques, it is demonstrated that microsurgeries in children and adults show similar success rates and complication rates [3]. Most past clinical reports, however, included a heterogeneous group of pediatric patients, involving variously different defect causes such as trauma, tumor, congenital malformation, scar contracture, etc. Also, most studies failed to focus on specific anatomic regions, including defects in head and neck, flank, and upper and lower extremities. Considering the importance of defect cause and location in determining surgical success, studies relying on heterogeneous population may have some limitations in drawing meaningful conclusions [1,3].
Compared with other causes like post-tumor resection, free flap on traumatic defects tends to show a lower success rate [1]. After trauma, it is hard to precisely assess the extent of vascular injuries due to anatomical distortions. Moreover, trauma is likely to induce secondary perivascular fibrosis and inflammation, leading to a higher rate of thrombotic complications after surgery [1]. However, few studies are focused on trauma-induced defects in children. Most of them include both elective free flap and replantation from multi-centered patient groups and did not make a direct comparison with corresponding adult groups [4]. Those studies narrowed down to trauma, and failed to focus specifically on hand defects [1,3,5-11].
In this study, we focused on the homogeneous pediatric population who had posttraumatic hand defects treated with free flap surgery in the past 10 years. Direct comparison was made between the clinical outcomes of the pediatric group of 39 patients and the adult group of 184 patients.
Methods
Ethics statement: This study design was approved by the Institutional Review Board of Gwangmyeong Sungae General Hospital (No. KIRB-2020-N-003). Written informed consent was obtained for publication of this report and accompanying images.
A retrospective study was conducted on 39 patients under the age of 17 years old, and 184 adult patients who received elective microsurgical reconstruction for coverage of trauma-induced hand defects between 2011 January and 2021 December (Table 1). The surgery was done in a single medical center by similar surgical procedures carried out by four senior surgeons.
Our exclusion criteria were free flaps performed for defects other than trauma, emergent replantation, and recipient sites other than hand. Clinical data collected included patient demographic data including body mass index (BMI), level of injury, donor site, flap size, the diameter of anastomosed artery and veins, use of vein graft, operation time, hospital day, flap survival, and complications (i.e., secondary operation, transfusion, emergent revision, infection, and donor-site complications) (Table 1). In addition, subgroup analysis was done for pediatric patients under the age of 8 years, and we compared them with the adult group.
Statistical analysis was done using Fisher exact test (or chi-square test) for categorical variables, and Mann-Whitney U-test was applied for continuous variables such as artery and vein diameter, operation time, or hospital day. Statistical significance was considered at p<0.05.
1. Intraoperative and postoperative care
Intraoperative heparinized saline was used for irrigation of vessels in all patients. For postoperative systemic anticoagulation, 120 mg/kg of heparin sodium injection (low molecular weight heparin; Hanlim Inc., Yongin, Korea) was infused for pediatric patients daily and 2,400 mg for the adult group. In addition, prostaglandin E1 (Eglandin; Mitsubishi Tanabe Pharma Inc., Osaka, Japan) was intravenously used for 1 week (2 µg/kg for the pediatric group and 10 µg for the adult group daily). There was no routine pain control for both the pediatric and adult groups, and intravenous antibiotics were applied for 2 weeks after the surgery. Immobilization by arm restraints was carried out for 1 week. Postoperative monitoring of flaps was done by direct clinical observation checking flap color, capillary refill, pinprick, and also by hand-held Doppler examination [3,12].
2. Demographics
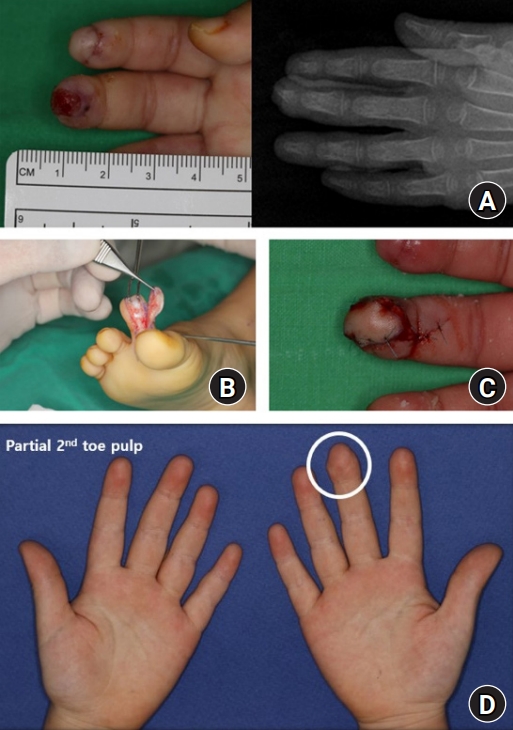
A total of 39 pediatric patients received 41 cases of free flap after hand trauma, and 184 adult patients received 184 cases from 2011 to 2021. The mean age of the pediatric group was 11 years old (12 months to 17 years old). The mean age of the adult group was 45 years old. Of the 39 pediatric patients, 34 were male (87.2%), similar to 160 male patients in the adult group (87.0%). The BMI of pediatric patients was 19.1 kg/m2, which falls under the normal range of the general pediatric population. Among the pediatric group, soft tissue defect was mostly at distal level (distal to distal interphalangeal [DIP] joint) with 25 cases, followed by nine cases in the middle level (DIP joint to proximal phalanx), and seven cases in proximal (metacarpophalangeal joint to hand). In the adult group, distal level soft tissue defects were in 86 cases, 42 cases in the middle, and 56 cases in the proximal level. Flap sizes of the pediatric group range from 1.3 to 108 cm2 (11.8 cm2 in average). Various types of donor sites were used in both groups, and a partial 2nd toe pulp-free flap was the most common donor site for both groups (Tables 1, 2). The mean±standard deviation of the follow-up period for the pediatric group was 12.4±3.1 months; and for the adult group, it was 19.1±5.6 months.
Results
1. Type of flaps
Fasciocutaneous flaps were predominantly used in both pediatric and adult groups, with partial 2nd toe free flaps (Fig. 1) accounting for 23 cases (56.1%) in the pediatric group and 84 cases (45.7%) in the adult group. In the pediatric group, osteocutaneous (2nd toe joint free flap), fascial (anterolateral thigh [ALT] fascial free flap), and musculocutaneous flap (anconeus muscle free flap) were used in one case each. Similarly, in the adult group, 11 cases were fascial flaps, which are followed by one osteocutaneous and one musculocutaneous flap each (Table 2).
2. Artery and vein diameter
The diameter of artery and vein anastomosed were measured by intraoperative photos during chart review. The mean artery diameter of pediatric patients was 0.58 mm (range, 0.2–1.0 mm), and the vein was 0.73 mm (range, 0.2–1.2 mm). This significantly decreased in the subgroup of patients under the age of 8 years. The mean artery diameter of the subgroup was 0.38 mm (range, 0.2–0.7 mm), and vein was 0.32 mm (range, 0.2–0.5 mm). As anticipated, the diameter increased in the adult group, with the mean artery diameter of 0.84 mm (range, 0.4–2.0 mm), and vein was 0.83 mm (range, 0.4–1.3 mm). Three groups (i.e., pediatric, subgroup, and adult) showed a significant increase in vessel diameters with age (p<0.001) (Tables 3-5).
4. Complications
Emergent reexploration was needed in two cases of the pediatric group (4.9%), with one arterial spasm and one arteriovenous thrombosis. Both cases were successfully salvaged after revision. There was no revision case in subgroup patients under the age of 8 years. In the adult group, 20 cases of revision were undergone (10.9%); but comparing this result with pediatric (p=0.383) and subgroup (p=0.369), these differences were not significant (Tables 3–5).
Secondary operations such as split-thickness skin graft, local flap, or stump revision were done in nine pediatric cases (22.0%), of which five were in the subgroup (35.7%). However, in the adult group, 123 cases of operations (66.8%) were needed, which split-thickness skin grafts accounted for the most (42.4%). Each difference between the pediatric group and the adult group (p<0.001) and between the subgroup and the adult group (p=0.022) was statistically significant. Adult patients more frequently needed secondary operations than pediatric and subgroup patients (Tables 3–5).
Infection was present in four cases in the pediatric group (9.8%); but all of them were superficial, requiring only systemic antibiotics for treatment. There was no infection in the subgroup. In the adult group, 18 cases were present in total (9.8%), with 17 superficial and one deep tissue infection which required surgical drainage. The difference in infection rate between the pediatric group and the adult group (p>0.999) and between the subgroup and the adult group (p=0.621) was not statistically significant (Tables 3–5).
Five pediatric patients needed transfusion after surgery (12.2%, p=0.158), and two of them were under the age of 8 years (p=0.204). On the other hand, 10 adult patients needed transfusion (5.4%) and these differences were also not significant (Tables 3–5).
The mean operation time was 188 minutes in the pediatric group (p=0.405) and 164 minutes in the subgroup (p=0.234). This was nearly the same in the adult group, which showed to be 184 minutes in length. In addition, the average hospital day for the pediatric group, the subgroup, and the adult group were 28.1, 28.4, and 35.3 days each. There was a significant difference in hospital days between the pediatric group and the adult group (p=0.002), but not with the subgroup (p=0.052) (Tables 4, 5).
Discussion
Initial concerns about the technical difficulties of small vessel size, higher vasospascity, and limitations in selecting appropriate donor sites surgeons have been reluctant to offer microsurgery for pediatric traumatic defects [3,7,9]. A number of studies proved that treatment outcomes are nearly the same as adults [3,5,6]. Nevertheless, most of these clinical reports included a rather heterogeneous patient group with defects caused by trauma to post-tumor resection, and with various anatomical locations [1].
Considering that free flap on traumatic defects tends to show a lower success rate than other defect causes, possibly due to posttraumatic anatomical distortions and secondary perivascular fibrosis and inflammation, it is highly valuable to sort out only trauma-induced cases and make a homogeneous analysis [1]. Moreover, since hand is relatively intricate by nature with smaller vessel diameters compared to other body parts, it seems that comparing the outcomes of a homogeneous pediatric population with hand defects with the corresponding adult population is meaningful.
Initially, it was believed that 0.7 mm is the lower limit of safe microscopic anastomosis in young children [1]. However, recent studies have shown high flap success rates of over 95% in children, which is similar to that of adults [13]. It is nowadays believed that generally, small vessel size does not necessarily lead to flap failure since the ‘relative size’ of a pediatric vessel is not smaller than adults [4,14]. Also, it is believed that vasospasm is not more common in children, partly because children usually have no vascular disease leaving the vessels as in a pristine state. Moreover, studies suggest that the immature pediatric vessel walls lack muscularis layers, hence less likely to cause vasospasm [4,6]. Our findings correspond to these beliefs since both pediatric and subgroup patients had no significant difference with adults in terms of emergent revision rates or flap survival rates, although with a marked difference in the diameters of vessels (Tables 4, 5).
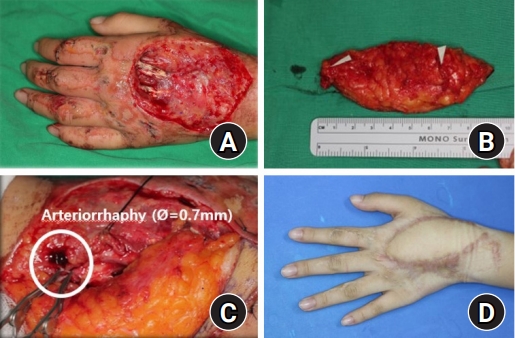
Previously, choosing the donor site was mainly focused on flap survival. Hence, donor sites with consistent anatomies such as rectus abdominis flap or latissimus dorsi muscle flaps were preferred. Recently the paradigm of donor selection has shifted to seeking ‘less donor morbidity,’ as high success rates were guaranteed [1,5,7,8]. Besides, the donor choice for children needs extra care due to high growth potential [10]. As a result, recently fasciocutaneous flaps and perforator-free flaps have become popular due to supple tissue volume, great growth potential, less donor morbidity, and the versatility to change into full-thickness skin grafts [7]. This recent trend resonates in our study as fasciocutaneous flaps such as venous forearm flap (Fig. 2) and perforator-free flaps such as ALT free flap (Fig. 3) accounted for a vast majority of both pediatric (56.1%) and adult group (45.7%). There were no donor-site complications for the pediatric group and only two cases of adult groups had donor dehiscence, which was managed by secondary closure. Although various types of flaps were used, there was an obvious preference for certain donor sites (i.e., 2nd toe pulp). This seems to contribute to a higher flap survival rate as a single surgical team gets more skilled after repeating the same type of surgery [2].
The only outcome that had a statistically significant difference between the three groups were secondary operations. Pediatric patients had only 21.9% of secondary operation rates, and subgroup patients under the age of 8 years, had 35.7% of STSG or local flaps. However, a much higher number of adult patients (67.4%) received secondary surgery. The reason might be that some adult patients have vasculopathies such as type 2 diabetes, hypertension, and atherosclerosis, while all pediatric patients have fully pristine vessel lumens [4,6]. Besides, since adult patients needed larger flaps, the larger flap size combined with hindersome blood flow may cause more partial necrotic changes around flap margins.
Infections were rare, with only four cases of pediatric patients and 17 cases of adult patients suffering minor superficial cellulitis. Only one case of the adult group suffered from deep tissue infection with purulent discharge. We were able to manage the deep tissue infection through serial aseptic dressings in the operation room [12].
Unlike the previous studies in which nearly 40% of pediatric patients needed transfusion [1], 12.2% of pediatric patients (14.3% of subgroup patients) and 5.4% of adult patients needed a transfusion. Although statistically insignificant, the subgroup had the highest rate and adults had the lowest rate of transfusion. This supports our belief that as smaller the body size and less body fluid, the more patients are prone to blood loss. However, the rate of transfusion may be biased, as the decision for initiating transfusion is subjective and the exact blood loss of each patient was not calculated.
The limitation of this study is the short follow-up period of pediatric group patients (12.4 months in average), which is not sufficient to fully assess the long-term functional outcomes. Due to this short follow-up period, we could not assess the donor and recipient growth. In addition, since this study relied on retrospective chart review, we could not objectively analyze the functional parameters such as 2-point discrimination sensory check, hand grip power, DASH (Disabilities of Arm, Shoulder and Hand) score, etc [1,13,15]. Moreover, although the surgical procedures were similar, the fact that operations were undergone by four different senior surgeons may present bias since the ‘surgeon factor’ is one of the most important factors in surgical outcomes. Finally, our age of patient selection was under 17 years old, similar to other reports [5,7,8,12]. However, there is a study claiming that the surgical technique and process of those over 10 years old are almost the same in adults [3]. Among 39 pediatric patients in our study, some of them may be not appropriate to represent pediatric physiology and anatomic features.
Conclusion
Microsurgical reconstruction for trauma-induced hand defects in the pediatric population may bring us a high success rate and low complication rate just as adults. The pediatric population may be more resistant to partial necrotic flap changes and require fewer secondary operations than adults do.