Introduction
Glomus tumors are benign hamartomas of the glomus body typically found in the distal phalanx or the subungual region in the reticular layer of the dermis. It is characterized by intractable pain around the nail and about 75% of glomus tumors are observed at the subungual area [1,2].
The specific location of glomus tumors within the finger has traditionally dictated the surgical approach for its eradication. Among the various surgical approaches devised for complete excision, the transungual approach is a common choice of tumors located in the subungual area [3]. In this approach, the nail plate is partially or completely removed, and excision is made by cutting through the nail bed over the tumor and repairing it after the eradication of the tumor. It may provide a good visual field to the tumor itself, however, yield cosmetically unsatisfying results with nail deformity if the nail bed is injured while removal of tumors or when suturing of the nail bed is made without care. Furthermore, when the incision site on the nail bed is not exactly matched over the tumor, it should be extended to find very tiny tumor [4].
Anatomically, the germinal matrix, which is located proximal to the nail bed, is responsible for 90% of nail growth [5]. Due to the characteristic location of the subungual glomus tumor, surgical excision of this tumor by cutting through the nail bed and matrix after the removal of the nail plate may cause injury to the nail bed and germinal matrix. Furthermore, the nail plate plays a pivotal role in protecting the underlying structures of the nail bed, germinal matrix, and bone. When the nail plate is removed and thus injured, the underlying structures are more prone to be exposed to the risk of infection, and the exposed structures may present as a source of postoperative pain.
Many surgical approaches to subungual glomus tumors have been introduced such as modified transungual and periungual approaches to skillfully remove the tumor [6-10]. In this study, we modified the traditional transungual approach not to need of removal of the nail plate and to avoid nail bed repair. The nail sparing and sub-nail bed approach may contribute to minimizing nail deformity by elevating the nail plate and the nail bed as a whole in an antegrade fashion.
Methods
1. Patients and clinical assessment
Ethics statement: The medical records of patients were retrospectively reviewed after obtaining the Institutional Review Board’s approval of Korea University College of Medicine (No. 2021AN0180). The study was performed in accordance with the Declaration of Helsinki, and written informed consent was waived due to its retrospective nature.
Inclusion criteria were patients with subungual glomus tumor of the finger who were treated with nail-sparing and sub-nail bed approach. All included patients presented with at least one of the classic symptom triad of glomus tumor. Pinpoint tenderness was assessed with Love’s pin test, and pain score was assessed using a visual analog scale (VAS, 0–10) [11]. Paroxysmal pain and the presence of cold insensitivity were assessed by asking the patient of pain and history of elicited pain in low temperatures. The subjective and objective results and final nail deformities were classified according to the grading system with respect to the nail deformity. Subjective grading was performed using a survey via telephone or outpatient visit, and the respective shapes of nails were photographed for evaluation at the time of the survey. The patient was asked if he or she were either “satisfied” with the outcome of the surgery or “unsatisfied.” Objective grading was performed by two orthopedic hand surgeons using preoperative and final follow-up photographs of the nails. They were classified as “excellent,” if there were improvements in nail shape after surgery (Fig. 1A). They were classified as “good,” if preoperatively normal nail shape remained normal after surgery or if there was no significant change in nail deformities seen postoperatively after surgery (Fig. 1B). They were classified as “poor,” if worsening of the nail shape was observed after surgery (Fig. 1C).
1. Surgical technique
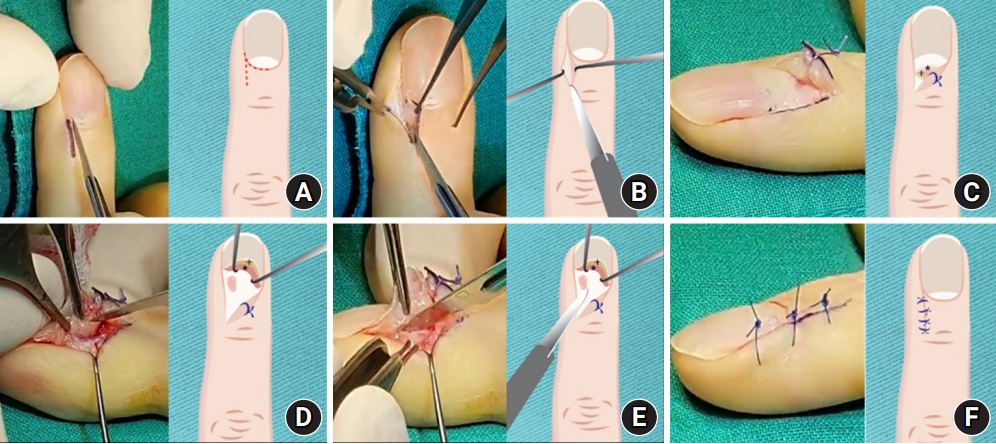
The preoperative diagnosis and approximation of the size and location of the glomus tumor were performed with the aid of 3.0-tesla magnetic resonance imaging (MRI). The area of most tenderness or discomfort was identified preoperatively and marked before the operation. All of the surgical procedures were performed under brachial plexus block anesthesia or local digital nerve block. Tourniquets were applied, limiting exsanguination to elevation of the extremity preventing the loss of color of the tumor from the normal surrounding tissue. Preoperative incision drawing was initially performed. A longitudinal incision from the proximal corner of the nail folds was created extending distally and proximally along the lateral border of the nail fold. This incision was made either on the radial or ulnar side of the finger depending on the eccentric location of the subungual tumor (Fig. 2A, 2B). Upon the exposure of the underlying structures, care was taken not to damage the underlying germinal matrix and nail bed as they are located slightly lateral to the proximal nail fold. The skin flap was further elevated until the proximal end of the nail bed and germinal matrix was fully exposed and the skin flap was subsequently fixed with a stay suture (Fig. 2C). The proximal end of the germinal matrix, nail bed, and nail plate were elevated in one layer from the underlying bone until complete exposure of the glomus tumor was achieved (Fig. 2D). After complete exposure of the tumor, no further elevation of germinal matrix, nail bed, and nail plate was needed. The tumor was then identified with the help of magnifying loupes with light. Typically, the margin of the glomus tumor is well-distinguished from the surrounding loose areolar tissue with its shiny and pinkish round contour. With a no. 15 blade, dissection of the tumor from the surrounding soft tissue was performed (Fig. 2E). After complete removal of the tumor, the germinal matrix, nail bed, and nail plate were placed back in their original position and the incised nail fold was repaired using a 4-0 nonabsorbable suture over the repositioned nail plate (Fig. 2F).
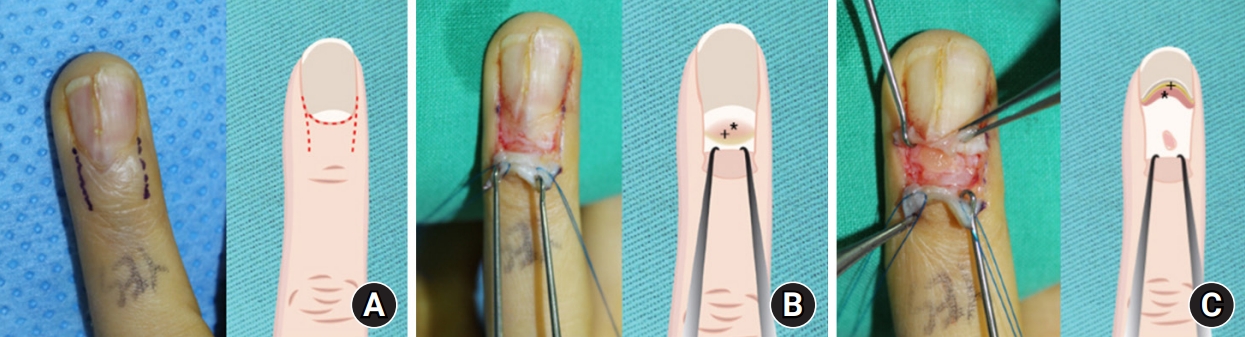
In cases where the tumor was located rather centrally, two horizontal and longitudinal incisions were created along both sides of the nail folds (Fig. 3A). Skin flaps were elevated until the exposure of the proximal nail bed and germinal matrix was achieved (Fig. 3B). From the proximal end of the germinal matrix, the nail bed and nail plate were elevated from the bone until full exposure of the underlying glomus tumor was obtained (Fig. 3C). After removal of the tumor, the elevated nail plate, nail bed, and germinal matrix were repositioned to their original sites and both nail folds were sutured meticulously with 4-0 nonabsorbable sutures.
Results
1. Patient demographics and clinical characteristics
Between June 2006 to May 2021, 29 patients were enrolled and treated using the nail-sparing and sub-nail bed approach for the excision of subungual glomus tumors and followed up for an average of 49.5 months (range, 6–179 months after surgery). One patient presented with tumors on four different fingers. Therefore, a total of 32 cases were evaluated. There were 11 male and 18 female patients in this study with ages ranging from 26 to 74 years (mean, 43.4 years). Preoperatively, all the patients complained of at least one of the classic symptom triads of glomus tumors, and 13 cases (40.6%) presented with various combined nail deformities. Cold intolerance was seen in 71.9% and paroxysmal pain was seen in 68.8% of patients. The glomus tumor was located eccentrically in the subungual area in 28 cases (87.5%), while four (12.5%) were located centrally. Twenty-one cases (65.6%) were located under the nail matrix, whereas the remaining 11 cases (34.4%) were located under the nail bed. The mean tumor diameter was 4.5 mm (range, 0.6 – 9.8 mm) (Table 1).
2. Preoperative and postoperative pain evaluation
All patients showed positive Love’s pin test. The mean VAS pain score before surgery was 7.0 (range, 5−9). All patients showed symptom relief after surgery, with a mean VAS pain score of 1.8 (range, 1–3) 1 week after the operation. At a mean follow-up of 49.5 months (range, 6–179 months), all patients showed pain relief with a mean VAS score of 0 (Table 2). There were no signs of any surgical complications such as any recurrence of tumors, digital nerve injury, and resultant paresthesia of the fingers after surgery at final follow-up.
3. Postoperative outcomes
All patients had complete recovery without recurrence of tumors. With respect to subjective cosmetic grading, 31 cases (28 patients) out of the 32 cases indicated the postoperative nail to be “satisfied”. One patient reported the postoperative nail to be “unsatisfied.”
Objective cosmetic gradings performed by two orthopedic hand surgeons were as follows: three out of the total cases (9.3%) were graded as “excellent” with marked improvement in nail shape after surgery and 28 cases (87.5%) were graded as “good.” All of the preoperatively normal shaped nails (n=19) remained normal after surgery; nine out of 10 cases with preoperative longitudinal grooves remained as longitudinal grooves after surgery. One case (3.1%) with preoperative longitudinal groove worsened as a longitudinal groove with streak and was graded as “poor.” This patient was the same person who subjectively claimed his nail shape to be “unsatisfactory” (Table 3).
Discussion
Glomus tumors are vascular neoplasms arising from a contractile neuromyoarterial structure found in the reticular dermis called the glomus body [12]. It is known to be only curable by the complete excision of the tumor. Depending on the location of the tumor, it can be approached and removed by ipsilateral or bilateral mid-lateral excisions if located in the pulp area [8]. However, approximately 75% of the tumors are located in the subungual area, and its proximity to the nail matrix and germinal matrix complicates surgical excision because it is likely to be damaged during the excision when using the traditional transungual approach [13-15]. Germinal matrix, which is located proximal to the nail bed, is responsible for 90% of nail growth. Although the classical direct transungual approach has been known to provide good visualization and easy access to the tumor [16], removal of nail takes time to regrow into a normal nail and risks further damaging the germinal matrix and nail bed [17]. In an attempt to avoid nail bed injury, lateral subperiosteal approach has been introduced where the tumor is removed by elevating a flap under the periosteum through a lateral incision of the nail bed [18]. However, this method is limited by the location of the tumor, and it may injure the digital nerves. Although the modified transungual nail preserving approach introduced by Lee et al. [17] offers preservation of the nail plate, recurrence of pain in some cases and surgical procedure of meticulous nail bed repair were limitations [17]. The modified periungual approach may be associated with a significant injury to the germinal matrix [8].
As described, the location of the tumor usually dictates the surgical approach. In this study, all of the tumors were located either peripherally or centrally near the germinal matrices in the more proximal aspect of the nail plate; therefore, the approach introduced in this study was adequate. We did not have any cases where the tumors were located far distally in the subungual area. For glomus tumors located rather distally in the subungual regions; we would assume that a similar approach starting distally beneath the nail bed could be utilized. If the tumor is located somewhere other than the subungual area such as in the pulp, a mid-lateral approach would be appropriate [8]. Patients with glomus tumors in the pulp were not enrolled in this study because the approach would not be indicated in such cases [8,19].
The nail-sparing and sub-nail bed approach that was used in this study lifted the germinal matrix and the nail plate as a whole and did not require suturing of the nail bed, and resulted in satisfactory cosmetic outcome without significant nail deformities after the operation. Nail bed sutures that are not performed meticulously may contribute to subsequent deformities and furthermore, foreign body reaction by the suture material increases the risk of infection [4]. Most importantly, nail regrowth due to nail removal and suturing of the germinal matrix as performed in the traditional transungual approach were avoided which may have contributed to higher patient satisfaction and decreased postoperative pain and infection. The elevation of the germinal matrix, nail bed, and the nail plate as a whole from the underlying bony cortex typically provided sufficient exposure of the tumor. With respect to postoperative recovery time, patients returned to normal daily activity after 2 weeks postoperative which is comparable to traditional 5 weeks with the transungual approach [20].
One case that was graded as “poor” objectively seemed to have had a couple of preoperative features that may have caused worsening of the cosmetic outcome. The size of the tumor was relatively large (approximately 0.7×0.5×0.3 cm3), and the nail bed and significant part of the germinal matrix were invaded, and underlying distal phalanx bony erosion was noted by the longstanding tumor mass. Furthermore, the patient’s duration of symptoms (pain and nail deformity) was approximately 7 years which is comparably longer than the mean duration of symptoms of 3.8 years as reported in a previous study [21]. Postoperative patient satisfaction and resultant nail deformity in one patient that presented with glomus tumors on four different fingers were excellent as she did not complain of any significant nail deformities in all four fingers and was satisfied with the cosmetic outcome. In general, solitary glomus tumors are known to be more common, while multiple glomus tumors can occur rarely in the digits [12].
There are several limitations to this study. We were unable to directly compare the results of other methods of operation such as the classical transungual approach performed by the same surgeon at one institution. Secondly, tumor recurrence was only defined based on the lack of persistent or recurring pain of the patient without comparing the preoperative and final follow-up MRIs. Finally, our data analyses may have contained recall bias as the medical records were retrospectively reviewed.